Thur Oct 27, 2011
Today's cases.
CASE 1,
A Shetland 6-month-old male had a firm lump on the right of the anus. "Perineal hernia?" I thought at first but it was not reduced in size when pushed inwards. No pain. "Suddenly appeared in the last 4 days," the young man said. So, what is it?
SEDATION
Zoletil 50 0.1 ml sedated lasted 5 minutes. No hyperextension of limbs. Isoflurane gas top up. Syringe out serous blood 4 ml. Incise. A capsule-like sac seen. 3/0 nylon stitched cross stitch x 1. Blood test showed no bacterial infection.
CASE 2.
8-year-old male shih Tzu with blood in both ears. After washing, I could see a large wart in left ear and numerous tumours in right ear. "No drugs can cure this dog," I said. "Surgery is required." Ideally ear canal ablation, not just excise the warts and lumps. "Wear an e-collar," I said as the owner did not wish to have the operation on financial considerations. Ringworm generalised and a small circum-anal tumour above anus.
Thursday, October 27, 2011
710. Follow up: Acute Tick fever in a young dog that went to a dog park
DRAFT CASE REPORT
DAY 1
Thursday, Oct 20, 2011
English Cocker, Male, 2 years, 11 kg
Dog eating less. Not active. The friend suggested taking the dog to see me.
I saw small ticks all over the body. The dog had been to a dog park in Pasir Ris recently/
Very pale gums. Blood test - low haemogloblin, low RBC and low platelets. Blood smear on Giemsa stain showed Babesia gibsoni. Ehrlichia seen. 0.5 ml Imizole (imidocarb) SC given. Dosage is 0.5 ml/10 kg.
IV dextrose and baytril. Vit K1 2 ml IV. Doxycycline 5mg/kg twice a day for 21 days. 10mg/kg twice a day had been proposed by some vet books but this is 4x the standard dose. Multivitamin paste. Vit K1 tablets (1/4 tab/day).
DAY 2
Friday, Oct 21, 2011
Gums still pale. No appetite. Vit K1 2 ml IV and supportive therapy. However the dog barks loudly when the owner came, exhausting himself. Owner brought his liver treats. He ate one.
Blood test results before Imizole 0.5 ml SC treatment:
Liver profile= Normal
Kidney profile= Normal
Hematology=
*Hemoglobin- 7g/dL [Normal range: 12-18]
*Red Blood Cells- 2.8 x10^12/L [Normal range: 5.5-8.5]
White Blood Cells- 13.2 x10^9/L [Normal range: 6-17]
*Packed Cell Volume= 0.19 [Normal range: 0.37-0.55]
Platelets= 52 [Normal range: 200-500]
*Nucleated Red Blood Cells seen [Severe demand for RBC to be release from Bone Marrow]
No platelet clump seen
--------------------------------------------------------------------------------
Blood test results 1 day after Imizole 0.5 ml SC treatment:
Liver profile= Enzymes increased
Kidney profile= Normal
Hematology=
*Hemoglobin- 7g/dL [Normal range: 12-18]
*Red Blood Cells- 2.9 x10^12/L [Normal range: 5.5-8.5]
White Blood Cells- 9.6 x10^9/L [Normal range: 6-17]
Packed Cell Volume= 0.2 [Normal range: 0.37-0.55]
*Platelets= 64 [Normal range: 200-500]
No platelet clump seen but few giant platelets present
-------------------------------------------------------------------
What is the importance of platelets?
a) Numbers:
The platelet count gives a general indication of the clotting ability of the blood. If the number of platelets falls below a certain critical level, spontaneous bleeding may occur. A low platelet count may indicate a problem with platelet production in the bone marrow, or may signal the presence of disease that is causing the platelets to be used up or destroyed. An increased platelet count often reflects excitement, exertion, or an activated bone marrow. In rare cases, an extremely high platelet count may indicate there is underlying bone marrow cancer.
b) Size:
The size of a platelet is related to its age; young platelets are large and plump, and older platelets are generally smaller. This can be important if the platelet count is low; the presence of large, plump, young platelets in the blood indicates that the bone marrow is functioning well, and is responding to the need for more platelets.
c) Appearance:
Very rarely, bizarre giant platelets, or abnormal immature platelets may be found, and these may signal the presence of an underlying bone marrow disorder or cancer
[Reference: http://www.fetchdog.com/learn-connect/dog-resource-library/health/diagnostic-tests/Complete-Blood-Count-for-Dogs/D/300600/P/1:5:55:601:6103/I/AR000010025]
DAY 3
Saturday, Oct 22, 2011
4PM
The owner came, her friend and the godfather. 2-hour visit. Loud barks.
At 7 pm, the 3 visitors left. The dog panted, heart beat very fast, as if he had run a sprint. It was bad. Would he die? I should have allowed a 10-minute visit, not 120 minutes!
Connected IV - glucose 100 ml, then dextrose saline with duphalytes 500 ml. Gave lasix IV. Atropine 0.5 ml IM. By the time I went home, it was past 7 pm.
The owner was prohibited from visiting for the next few days. This dog had a keen hearing as he could hear the owner's voice at the reception area some distance away in the back of the Surgery and started barking non-stop for several minutes.
DAY 4
Sunday, Oct 23, 2011
Morning 10 am. Dog felt well. Barking for a while. Smelt food. Not eating. Hand fed A/D canned food and given water and electrolytes.
DAY 5.
Monday, Oct 24, 2011
IV drip. Blood looked reddish unlike bluish blood for past few days. Good news.
Passed normal stools when taken out.
DAY 6.
Tuesday, Oct 25, 2011
Deepavali. Public holiday.
Alert and standing in cage. I am relieved that the gum looks pinker. Blood test at another lab showed normal platelets but still very low Hb and RBC. I phoned owner to take the dog home at 6 pm to be nursed by owner.
DAY 7.
Wednesday, Oct 26, 2011
At home. With iron tablets and good food including egg yolk and liver.
DAY 8.
Thursday, Oct 27, 2011
At home. I phoned the owner at 6.30 pm
"My dog is very active, hungry and thirsty. I found two ticks, a grey one on her body. I put tick powder onto my bed area." One tube Advantix Spot on had been applied on Day 6. Yet he had two ticks stuck in skin. Otherwise appeared normal.
-------------------------------------------------------------------------------------------------------------
Scheduled Appointments
DAY 9
Friday, Oct 28, 2011
DAY 11
Sunday, Oct 30, 2011
Scheduled for next Imizole (imidocarb) injection SC. Babesia and Ehrlichia seen on 2nd blood smear on Day 6. Possibly has anaplasmosis?
DAY 12
Monday, Oct 31, 2011
Urine to be collected by the owner for urinalysis.
Acute tick fever needs regular monitoring till negative blood test results 2 weeks after the previous test but most owners don't have the time to do so.
DAY 1
Thursday, Oct 20, 2011
English Cocker, Male, 2 years, 11 kg
Dog eating less. Not active. The friend suggested taking the dog to see me.
I saw small ticks all over the body. The dog had been to a dog park in Pasir Ris recently/
Very pale gums. Blood test - low haemogloblin, low RBC and low platelets. Blood smear on Giemsa stain showed Babesia gibsoni. Ehrlichia seen. 0.5 ml Imizole (imidocarb) SC given. Dosage is 0.5 ml/10 kg.
IV dextrose and baytril. Vit K1 2 ml IV. Doxycycline 5mg/kg twice a day for 21 days. 10mg/kg twice a day had been proposed by some vet books but this is 4x the standard dose. Multivitamin paste. Vit K1 tablets (1/4 tab/day).
DAY 2
Friday, Oct 21, 2011
Gums still pale. No appetite. Vit K1 2 ml IV and supportive therapy. However the dog barks loudly when the owner came, exhausting himself. Owner brought his liver treats. He ate one.
Blood test results before Imizole 0.5 ml SC treatment:
Liver profile= Normal
Kidney profile= Normal
Hematology=
*Hemoglobin- 7g/dL [Normal range: 12-18]
*Red Blood Cells- 2.8 x10^12/L [Normal range: 5.5-8.5]
White Blood Cells- 13.2 x10^9/L [Normal range: 6-17]
*Packed Cell Volume= 0.19 [Normal range: 0.37-0.55]
Platelets= 52 [Normal range: 200-500]
*Nucleated Red Blood Cells seen [Severe demand for RBC to be release from Bone Marrow]
No platelet clump seen
--------------------------------------------------------------------------------
Blood test results 1 day after Imizole 0.5 ml SC treatment:
Liver profile= Enzymes increased
Kidney profile= Normal
Hematology=
*Hemoglobin- 7g/dL [Normal range: 12-18]
*Red Blood Cells- 2.9 x10^12/L [Normal range: 5.5-8.5]
White Blood Cells- 9.6 x10^9/L [Normal range: 6-17]
Packed Cell Volume= 0.2 [Normal range: 0.37-0.55]
*Platelets= 64 [Normal range: 200-500]
No platelet clump seen but few giant platelets present
-------------------------------------------------------------------
What is the importance of platelets?
a) Numbers:
The platelet count gives a general indication of the clotting ability of the blood. If the number of platelets falls below a certain critical level, spontaneous bleeding may occur. A low platelet count may indicate a problem with platelet production in the bone marrow, or may signal the presence of disease that is causing the platelets to be used up or destroyed. An increased platelet count often reflects excitement, exertion, or an activated bone marrow. In rare cases, an extremely high platelet count may indicate there is underlying bone marrow cancer.
b) Size:
The size of a platelet is related to its age; young platelets are large and plump, and older platelets are generally smaller. This can be important if the platelet count is low; the presence of large, plump, young platelets in the blood indicates that the bone marrow is functioning well, and is responding to the need for more platelets.
c) Appearance:
Very rarely, bizarre giant platelets, or abnormal immature platelets may be found, and these may signal the presence of an underlying bone marrow disorder or cancer
[Reference: http://www.fetchdog.com/learn-connect/dog-resource-library/health/diagnostic-tests/Complete-Blood-Count-for-Dogs/D/300600/P/1:5:55:601:6103/I/AR000010025]
DAY 3
Saturday, Oct 22, 2011
4PM
The owner came, her friend and the godfather. 2-hour visit. Loud barks.
At 7 pm, the 3 visitors left. The dog panted, heart beat very fast, as if he had run a sprint. It was bad. Would he die? I should have allowed a 10-minute visit, not 120 minutes!
Connected IV - glucose 100 ml, then dextrose saline with duphalytes 500 ml. Gave lasix IV. Atropine 0.5 ml IM. By the time I went home, it was past 7 pm.
The owner was prohibited from visiting for the next few days. This dog had a keen hearing as he could hear the owner's voice at the reception area some distance away in the back of the Surgery and started barking non-stop for several minutes.
DAY 4
Sunday, Oct 23, 2011
Morning 10 am. Dog felt well. Barking for a while. Smelt food. Not eating. Hand fed A/D canned food and given water and electrolytes.
DAY 5.
Monday, Oct 24, 2011
IV drip. Blood looked reddish unlike bluish blood for past few days. Good news.
Passed normal stools when taken out.
DAY 6.
Tuesday, Oct 25, 2011
Deepavali. Public holiday.
Alert and standing in cage. I am relieved that the gum looks pinker. Blood test at another lab showed normal platelets but still very low Hb and RBC. I phoned owner to take the dog home at 6 pm to be nursed by owner.
DAY 7.
Wednesday, Oct 26, 2011
At home. With iron tablets and good food including egg yolk and liver.
DAY 8.
Thursday, Oct 27, 2011
At home. I phoned the owner at 6.30 pm
"My dog is very active, hungry and thirsty. I found two ticks, a grey one on her body. I put tick powder onto my bed area." One tube Advantix Spot on had been applied on Day 6. Yet he had two ticks stuck in skin. Otherwise appeared normal.
-------------------------------------------------------------------------------------------------------------
Scheduled Appointments
DAY 9
Friday, Oct 28, 2011
DAY 11
Sunday, Oct 30, 2011
Scheduled for next Imizole (imidocarb) injection SC. Babesia and Ehrlichia seen on 2nd blood smear on Day 6. Possibly has anaplasmosis?
DAY 12
Monday, Oct 31, 2011
Urine to be collected by the owner for urinalysis.
Acute tick fever needs regular monitoring till negative blood test results 2 weeks after the previous test but most owners don't have the time to do so.
709. Neoderm for 2 months thins the 6-month-old shetland dog's skin
Oct 27, 2011
SOME INTERESTING CASES
I was on duty today and the young man came with a 5 kg thin Shetland with a big right perineal swelling of 4 days. Firm but not painful. Around 3 cm x 3 cm. So, what was it? A perineal hernia? No, as it cannot be pushed in. A haematoma or abscess? Likely. Zoletil 50 0.1 + 0.4 ml saline ml IV sedated the dog.
No hyperextension and therefore no need atropine unlike the Westie (pus in ears, consulted Vet 1 with no success, owner referred by an old client to me) last week when I gave him the same Zoletil 0.1 ml IV. He had stiff limbs which relaxed when I gave atropine 0.5 ml IM and gave ear irrigation. Pus and debris esp. right ear. No head-shaking 3 days after treatment
"My shetland's skin disease did not get cured," the young man of 20 years with 4 months left of National Service said. "I read in the internet that he may be suffering from demodecosis. The vet scraped his nose skin but found nothing. He gave me a Neodern cream to apply."
Two front paws near the dew claws were bald. I could see thinning of the skin and the tendons and bones below. Other parts of both the front paw look moth-bitten with hairless squares and circles. Both lower elbows ventral surface were bald.
I saw redness in skin below the front paws but not the back paws, took a hair microscopic exam and showed the young man ringworm. The other hairless area did not have ringworm as Neoderm had killed any fungus and also thinned the skin.
"My dog licks away everytime I apply Neoderm," he said of the hairless elbow and armpits.
"How long you had applied?" I asked.
"Two months," he said. I asked him to stop Neoderm as it thins the skin when used too long. Prescribed anti-fungal tablets and wash and review in 2 weeks. Should recover. Demodex unlikely.
I showed Dr Vanessa the effects of Neoderm. "This is the reason I seldom prescribe Neoderm," I said. "The owner uses it for a long time, thinning the skin."
SOME INTERESTING CASES
I was on duty today and the young man came with a 5 kg thin Shetland with a big right perineal swelling of 4 days. Firm but not painful. Around 3 cm x 3 cm. So, what was it? A perineal hernia? No, as it cannot be pushed in. A haematoma or abscess? Likely. Zoletil 50 0.1 + 0.4 ml saline ml IV sedated the dog.
No hyperextension and therefore no need atropine unlike the Westie (pus in ears, consulted Vet 1 with no success, owner referred by an old client to me) last week when I gave him the same Zoletil 0.1 ml IV. He had stiff limbs which relaxed when I gave atropine 0.5 ml IM and gave ear irrigation. Pus and debris esp. right ear. No head-shaking 3 days after treatment
"My shetland's skin disease did not get cured," the young man of 20 years with 4 months left of National Service said. "I read in the internet that he may be suffering from demodecosis. The vet scraped his nose skin but found nothing. He gave me a Neodern cream to apply."
Two front paws near the dew claws were bald. I could see thinning of the skin and the tendons and bones below. Other parts of both the front paw look moth-bitten with hairless squares and circles. Both lower elbows ventral surface were bald.
I saw redness in skin below the front paws but not the back paws, took a hair microscopic exam and showed the young man ringworm. The other hairless area did not have ringworm as Neoderm had killed any fungus and also thinned the skin.
"My dog licks away everytime I apply Neoderm," he said of the hairless elbow and armpits.
"How long you had applied?" I asked.
"Two months," he said. I asked him to stop Neoderm as it thins the skin when used too long. Prescribed anti-fungal tablets and wash and review in 2 weeks. Should recover. Demodex unlikely.
I showed Dr Vanessa the effects of Neoderm. "This is the reason I seldom prescribe Neoderm," I said. "The owner uses it for a long time, thinning the skin."
Wednesday, October 26, 2011
708. Script for "skin disease in a dwarf hamster" video to educate pet owners
Skin Diseases In A Dwarf Hamster
Dr Sing Kong Yuen, BVMS (Glasgow), MRCVS
26 October, 2011
toapayohvets.com
Be Kind To Pets
Veterinary Education
Project 2010-0129
THE HOOK - A ROBOROVSKI HAMSTER CAN'T STOP SCRATCHING

The 10-year-old caregiver asks mum many times: "Please go to the vet." Mum has no time. (Show busy Singaporean mum with two jobs at workplace if possible, taking MRT, bus etc)
Bringing Veterinary Knowledge Alive To Vet Students & Pet Owners - Sponsored by
Toa Payoh Vets --- toapayohvets.com
26 October, 2011
INTRODUCTION - hamster bites himself. More self-biting wounds - to treat or not to treat?
If not treated - consequences - cellulitis and death
10-year-old girl is worried.
MIDDLE - Picture of cage and home?
what the mother does, what the vet does, what the vet groomer does? Images show hamster has been clipped short by the groomer. Ready for bathing. How do you bathe a hamster?
HOW TO BATHE A HAMSTER - VIDEO
Will hamster drown? Hamsters are usually given sand-bath (picture of hamster doing a sand bath) by pet owners. But now, he needs a water bath. What to do? How to bathe him? Video "How-to"
POST-BATHING - GOES HOME. Medication, bathing and new bedding. Hygiene of cage.
Check out example at: Oro-nasal fistula in the dog
http://www.youtube.com/user/99pups#p/u/1/5AWHpWYWgy4
CONCLUSION - Pictures of other hamsters with skin diseases to be provided by Dr Sing
Early treatment of skin diseases means
earlier recovery, lower veterinary cost and more peace of mind to your child who cares for the hamster
For more information
please visit: www.toapayohvets.com, +65 9668-6468, 6254-3326, e-mail judy@toapayohvets.com
CREDITS.
Concept by: Dr Sing Kong Yuen
Video and narration by:
NO copyrighted music or audio to be inside this video
BE KIND TO DOGS & CATS --- GET EYE ULCERS TREATED WITHIN 4 HOURS --- IF YOU DON'T WANT THEM TO BE BLIND. More case studies, goto: Cats or Dogs
To make an appointment: e-mail judy@toapayohvets.com
tel: +65 9668-6469, 6254-3326
toapayohvets.com
Be Kind To Pets
Veterinary Education
Project 2010-0129
Webpage at:
http://www.sinpets.com/F6/20111037roborovski-dermatitis-skin-disease-singapore-toapayohvets.htm
Dr Sing Kong Yuen, BVMS (Glasgow), MRCVS
26 October, 2011
toapayohvets.com
Be Kind To Pets
Veterinary Education
Project 2010-0129
THE HOOK - A ROBOROVSKI HAMSTER CAN'T STOP SCRATCHING

The 10-year-old caregiver asks mum many times: "Please go to the vet." Mum has no time. (Show busy Singaporean mum with two jobs at workplace if possible, taking MRT, bus etc)
Bringing Veterinary Knowledge Alive To Vet Students & Pet Owners - Sponsored by
Toa Payoh Vets --- toapayohvets.com
26 October, 2011
INTRODUCTION - hamster bites himself. More self-biting wounds - to treat or not to treat?
If not treated - consequences - cellulitis and death
10-year-old girl is worried.
MIDDLE - Picture of cage and home?
what the mother does, what the vet does, what the vet groomer does? Images show hamster has been clipped short by the groomer. Ready for bathing. How do you bathe a hamster?
HOW TO BATHE A HAMSTER - VIDEO
Will hamster drown? Hamsters are usually given sand-bath (picture of hamster doing a sand bath) by pet owners. But now, he needs a water bath. What to do? How to bathe him? Video "How-to"
POST-BATHING - GOES HOME. Medication, bathing and new bedding. Hygiene of cage.
Check out example at: Oro-nasal fistula in the dog
http://www.youtube.com/user/99pups#p/u/1/5AWHpWYWgy4
CONCLUSION - Pictures of other hamsters with skin diseases to be provided by Dr Sing
Early treatment of skin diseases means
earlier recovery, lower veterinary cost and more peace of mind to your child who cares for the hamster
For more information
please visit: www.toapayohvets.com, +65 9668-6468, 6254-3326, e-mail judy@toapayohvets.com
CREDITS.
Concept by: Dr Sing Kong Yuen
Video and narration by:
NO copyrighted music or audio to be inside this video
BE KIND TO DOGS & CATS --- GET EYE ULCERS TREATED WITHIN 4 HOURS --- IF YOU DON'T WANT THEM TO BE BLIND. More case studies, goto: Cats or Dogs
To make an appointment: e-mail judy@toapayohvets.com
tel: +65 9668-6469, 6254-3326
toapayohvets.com
Be Kind To Pets
Veterinary Education
Project 2010-0129
Webpage at:
http://www.sinpets.com/F6/20111037roborovski-dermatitis-skin-disease-singapore-toapayohvets.htm
707. Producing the educational hamster skin disease video - comments by Dr Sing
Oct 26, 2011
I am producing a video for the AVA Responsible Pet Ownership Roadshow 2011 in Nov 2011 and time is running out. Below is my comment on the production!
Thank you for your two videos. Good hands-on work done on both videos. It is only by doing that one can learn and improve and I am glad you did that. Below are my comments.
GENERAL COMMENTS FOR HAMSTER VIDEO WHICH IS ATTENTION-GETTING
1. Hamster video introduction. Excellent narrative of daughter and mother. It captures the attention of the viewer.
2. Sequence is not correct as your starting scene is that of a hamster with its hair already clipped. Then you show scenes with a hamster with hair. Then, hair clipped, then a hamster with hair. Correct sequence is shown in www.toapayohvets.com front page but I will give you a webpage address when I produce the draft.
3. The point of view is that of the little girl who is worried about her hamster with skin disease. Because she is little, she can't go to the vet by herself. So she need to ask the mother for help.
So, the introduction, middle (at least 5 messages on a hamster's skin diseases) and conclusion will be from the little girl's point of view and her actions. Did she achieve her mission?
If she fails to get her mother to act, the hamster's self biting wounds will become skin infections with pus-producing bacteria (show another hamster with cellulitis from one of my cases). By then, it will be too late.
Why did the mother act? One reason is that the examinations are on-growing. The daughter's worries distract her from studying. So she goes to the vet. "The hamster needs to be hospitalised for 3 days to be treated," I said. "That will be fine, as my daughter is having her examinations!"
The side characters are the mother, the vet (consultation by the mother, diagnosis and treatment) and the groomer (clipping coat, bathing time, bathing).
4. Try NOT to superimpose text onto the character (e.g. onto the labrador's body) as this spoil the enjoyment of viewing of the animal.
This is an example from me:
THE HOOK
A roborovski (with hair)
http://www.kongyuensing.com/cgi/20111083dwarf-hamster-roborovski-scales-dandruff-skin-ulcers-toapayohvets-singapore.jpg
e.g. narrative from little girl. Show hamster moving if you have the video before clipping the hair
http://www.kongyuensing.com/cgi/20111085dwarf-hamster-roborovski-scales-dandruff-skin-ulcers-toapayohvets-singapore.jpg
CONCLUSION. The daughter phones the vet two times after bathing: "When can my hamster come home?" After bathing, on day 4 after hospitalisation, the mother brings the hamster. The 10-year-old girl is very happy.
ADVICES FROM DR SING
1. "Do not use the sharp pelleted litter as bedding," I said. "Use the soft paper type". Show cage with pelleted litter usually used for cats, covering part of the floor. Show cage with paper bedding covering the whole floor.
"But the other vet said that it is best not to change the bedding as it will stress out the hamster!"
"No two vets offer the same advices," I said. "In this case, the active roborovski hamster's body could have been scratched by the sharp ends of those pellets and bacterial infection of the skin causes itchiness and scratching!"
2. "Keep the cage floor clean," I advised.
Generally, the story must flow smoothly with actions preferred. The "clock" scene needs to be removed as it does not help since the timing is still 12 o'clock every time you flash this scene. No time movement!
FOR THE EAR IRRIGATION VIDEO
1. Do not superimpose text onto the body of the dog as it makes it less enjoyable to view the video.
2. Repetition of same scene. I note that ear scoping scene has been shown twice.
3. The video needs a hook which I spoke to you about. An action of the dog intensely scratching.
I have spoken to you earlier about this production.
Keep up the good work.
ADVICES
Try to use similar light text and black background as in the "Attack The Block"
trailer at:
http://www.youtube.com/results?search_query=attack+the+block+trailer&aq=1&oq=Att
Also adapt some of the stories and sounds but not copy their sounds, the story telling and the hook.
e.g. "Better call the police," the girl said
"You are better off calling the ghost-buster!"
e.g. In this hamster video narrative,you may think of above lines and replace "police" with "groomer" and "ghost-buster" with "vet"
I am producing a video for the AVA Responsible Pet Ownership Roadshow 2011 in Nov 2011 and time is running out. Below is my comment on the production!
Thank you for your two videos. Good hands-on work done on both videos. It is only by doing that one can learn and improve and I am glad you did that. Below are my comments.
GENERAL COMMENTS FOR HAMSTER VIDEO WHICH IS ATTENTION-GETTING
1. Hamster video introduction. Excellent narrative of daughter and mother. It captures the attention of the viewer.
2. Sequence is not correct as your starting scene is that of a hamster with its hair already clipped. Then you show scenes with a hamster with hair. Then, hair clipped, then a hamster with hair. Correct sequence is shown in www.toapayohvets.com front page but I will give you a webpage address when I produce the draft.
3. The point of view is that of the little girl who is worried about her hamster with skin disease. Because she is little, she can't go to the vet by herself. So she need to ask the mother for help.
So, the introduction, middle (at least 5 messages on a hamster's skin diseases) and conclusion will be from the little girl's point of view and her actions. Did she achieve her mission?
If she fails to get her mother to act, the hamster's self biting wounds will become skin infections with pus-producing bacteria (show another hamster with cellulitis from one of my cases). By then, it will be too late.
Why did the mother act? One reason is that the examinations are on-growing. The daughter's worries distract her from studying. So she goes to the vet. "The hamster needs to be hospitalised for 3 days to be treated," I said. "That will be fine, as my daughter is having her examinations!"
The side characters are the mother, the vet (consultation by the mother, diagnosis and treatment) and the groomer (clipping coat, bathing time, bathing).
4. Try NOT to superimpose text onto the character (e.g. onto the labrador's body) as this spoil the enjoyment of viewing of the animal.
This is an example from me:
THE HOOK
A roborovski (with hair)
http://www.kongyuensing.com/cgi/20111083dwarf-hamster-roborovski-scales-dandruff-skin-ulcers-toapayohvets-singapore.jpg
e.g. narrative from little girl. Show hamster moving if you have the video before clipping the hair
http://www.kongyuensing.com/cgi/20111085dwarf-hamster-roborovski-scales-dandruff-skin-ulcers-toapayohvets-singapore.jpg
CONCLUSION. The daughter phones the vet two times after bathing: "When can my hamster come home?" After bathing, on day 4 after hospitalisation, the mother brings the hamster. The 10-year-old girl is very happy.
ADVICES FROM DR SING
1. "Do not use the sharp pelleted litter as bedding," I said. "Use the soft paper type". Show cage with pelleted litter usually used for cats, covering part of the floor. Show cage with paper bedding covering the whole floor.
"But the other vet said that it is best not to change the bedding as it will stress out the hamster!"
"No two vets offer the same advices," I said. "In this case, the active roborovski hamster's body could have been scratched by the sharp ends of those pellets and bacterial infection of the skin causes itchiness and scratching!"
2. "Keep the cage floor clean," I advised.
Generally, the story must flow smoothly with actions preferred. The "clock" scene needs to be removed as it does not help since the timing is still 12 o'clock every time you flash this scene. No time movement!
FOR THE EAR IRRIGATION VIDEO
1. Do not superimpose text onto the body of the dog as it makes it less enjoyable to view the video.
2. Repetition of same scene. I note that ear scoping scene has been shown twice.
3. The video needs a hook which I spoke to you about. An action of the dog intensely scratching.
I have spoken to you earlier about this production.
Keep up the good work.
ADVICES
Try to use similar light text and black background as in the "Attack The Block"
trailer at:
http://www.youtube.com/results?search_query=attack+the+block+trailer&aq=1&oq=Att
Also adapt some of the stories and sounds but not copy their sounds, the story telling and the hook.
e.g. "Better call the police," the girl said
"You are better off calling the ghost-buster!"
e.g. In this hamster video narrative,you may think of above lines and replace "police" with "groomer" and "ghost-buster" with "vet"
Tuesday, October 25, 2011
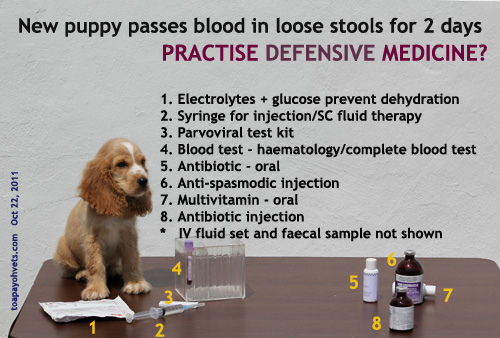
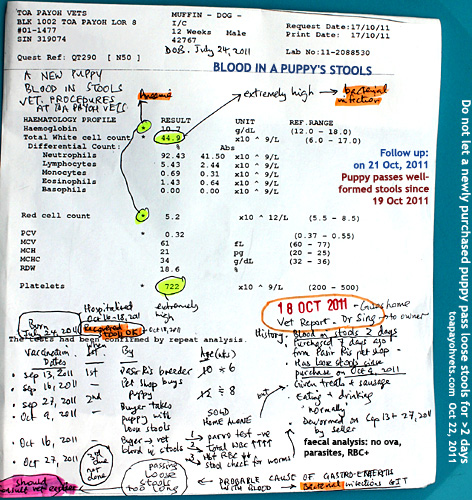
706. Practise defensive medicine? New puppy with blood in the stools
A NEW PUPPY WITH BLOOD IN THE STOOLS OR VOMITING AND DIARRHOEA
PROCEDURES AT TOA PAYOH VETS

When a new puppy has blood in the stools or vomiting/diarrhoea, the following will be the procedures at Toa Payoh Vets to provide the highest standard of care and to defend the vet in the event of litigation or complaint when the puppy dies later.
1. HISTORY. Record all vaccinations done and dates and by whom. Do not forget to do so. Record your epidemiological study to determine whether parvovirus is a likely cause.
2. GENERAL EXAMINATION. Demeanour. Weight, rectal temperature, pulse and respiratory rate. Abdominal pain, gas in the GIT and other observations.
3. DETAILED EXAMINATION. Parvoviral test, blood test (haematology or complete blood test), stool test. It will be a case for veterinary negligence if the parvoviral test is not done.

4. TREATMENT. According to symptoms. IV, SC or oral fluid therapy depending on situation. Antispasmodic, antibiotics, multivitamins, protein drip, Vit K1 when necessary. Times and amounts given will be recorded.

The vet in charge of the case is responsible for details of time, amount and other information will be recorded in the hospitalisation sheet.
5. COMMUNICATIONS WITH THE OWNER IN WRITING. A veterinary report explaining the significance of the tests and case must be given to the owner on discharge/death of the puppy. It is best to keep the owner informed daily of the health of the puppy. Such phone calls must be recorded in the medical case files.

Record under AMD (Against Medical Advice) the owner's rejection of advices of the test in your medical record. Failure to do so implies that the vet has not advised at all in cases of litigation/complaint. As Singapore is becoming a litigious society, I advise that the highest standard of care to be given at all times. An example of a case done by me is down shown in the images.
Updates and more pictures are at: TOA PAYOH VETS WEBPAGE:
http://www.sinpets.com/dogs/20111036puppy-blood-in-stools-diarrhoea-vomiting-singapore-toapayohvets.htm
PROCEDURES AT TOA PAYOH VETS

When a new puppy has blood in the stools or vomiting/diarrhoea, the following will be the procedures at Toa Payoh Vets to provide the highest standard of care and to defend the vet in the event of litigation or complaint when the puppy dies later.
1. HISTORY. Record all vaccinations done and dates and by whom. Do not forget to do so. Record your epidemiological study to determine whether parvovirus is a likely cause.
2. GENERAL EXAMINATION. Demeanour. Weight, rectal temperature, pulse and respiratory rate. Abdominal pain, gas in the GIT and other observations.
3. DETAILED EXAMINATION. Parvoviral test, blood test (haematology or complete blood test), stool test. It will be a case for veterinary negligence if the parvoviral test is not done.
4. TREATMENT. According to symptoms. IV, SC or oral fluid therapy depending on situation. Antispasmodic, antibiotics, multivitamins, protein drip, Vit K1 when necessary. Times and amounts given will be recorded.

The vet in charge of the case is responsible for details of time, amount and other information will be recorded in the hospitalisation sheet.
5. COMMUNICATIONS WITH THE OWNER IN WRITING. A veterinary report explaining the significance of the tests and case must be given to the owner on discharge/death of the puppy. It is best to keep the owner informed daily of the health of the puppy. Such phone calls must be recorded in the medical case files.
Record under AMD (Against Medical Advice) the owner's rejection of advices of the test in your medical record. Failure to do so implies that the vet has not advised at all in cases of litigation/complaint. As Singapore is becoming a litigious society, I advise that the highest standard of care to be given at all times. An example of a case done by me is down shown in the images.
Updates and more pictures are at: TOA PAYOH VETS WEBPAGE:
http://www.sinpets.com/dogs/20111036puppy-blood-in-stools-diarrhoea-vomiting-singapore-toapayohvets.htm
705. Post-op discharge 3 days after a breast tumour surgery
Yesterday, Oct 24, 2011, the lady owner brought her dog back as there was a "leakage" of reddish-brown fluid from the surgical wound. She had asked for advice over the phone but I told her that it would be hard to know what was happening. However the dog was eating.

"It is not possible for the dog to lick her wound," the lady said since her dog was wearing an E-collar post-operation. "I don't see my dog licking the wound when I am with her."
"I have seen cases where it has been done," I did now want to argue as most owners seem to think that the dog would lick the surgical wound in their presence. If not, then, the dog had not done it. Unless the e-collar is of a size so big, the dog can still lick its surgical wounds partly.
One of the stitches had a gap and post-op blood had leaked out. It was not serious. So, I hospitalised the dog for 3 days as she was walking at home. "Not much walking as she always lay down," the owner said.
"Any walking other than crate confinement will put tension on this long surgical wound," I said. "This is not a small 2-cm wound but more than 20-cm long. Good communication with the owner is important but sometimes it can test a vet's patience.
TIPS
In this case, I had not performed the surgery. However, I had discussed in my previous article that the "walk-in" sutures and horizontal mattress sutures on the skin would have given a tighter fit to control bleeding and prevent "leaking" of plasma. As each vet has his or her own skill and style in stitching up, it is difficult to say whether the subcutaneous stitching of the tissue and then simple interrupted skin sutures did permit "leakage" as there are many factors involved in a post-operation bleeding. In this case, the whole lower part of the dog's body was wet with the reddish brown plasma and blood. I asked Min to bathe the dog as her front leg skin and elbows had yellow flakes and this has nothing to do with the surgery. The dog had not been groomed.
"It is not possible for the dog to lick her wound," the lady said since her dog was wearing an E-collar post-operation. "I don't see my dog licking the wound when I am with her."
"I have seen cases where it has been done," I did now want to argue as most owners seem to think that the dog would lick the surgical wound in their presence. If not, then, the dog had not done it. Unless the e-collar is of a size so big, the dog can still lick its surgical wounds partly.
One of the stitches had a gap and post-op blood had leaked out. It was not serious. So, I hospitalised the dog for 3 days as she was walking at home. "Not much walking as she always lay down," the owner said.
"Any walking other than crate confinement will put tension on this long surgical wound," I said. "This is not a small 2-cm wound but more than 20-cm long. Good communication with the owner is important but sometimes it can test a vet's patience.
TIPS
In this case, I had not performed the surgery. However, I had discussed in my previous article that the "walk-in" sutures and horizontal mattress sutures on the skin would have given a tighter fit to control bleeding and prevent "leaking" of plasma. As each vet has his or her own skill and style in stitching up, it is difficult to say whether the subcutaneous stitching of the tissue and then simple interrupted skin sutures did permit "leakage" as there are many factors involved in a post-operation bleeding. In this case, the whole lower part of the dog's body was wet with the reddish brown plasma and blood. I asked Min to bathe the dog as her front leg skin and elbows had yellow flakes and this has nothing to do with the surgery. The dog had not been groomed.
704. Follow up on ptergium, glaucoma and enucleation of eye dog
Yesterday, Oct 24, 2011, I phoned the lady owner to enquire about her dog after eye enucleation. She was very happy as the dog was normal.
"Any bleeding from the eye?" I asked as there was some swelling of the stitched eye socket 3 hours after removal of the eyeball. In this case, I had stitched the conjunctival (upper and lower) tissues with 2/0 absorbable. Then I stitched the eyelid margins (as shown in the picture) with 3/0 nylon. So, there were two layers to prevent bleeding out of the eye.

"Some bleeding on the first day, but nothing serious. My dog is eating. I will see you 14 days later to remove the stitches."
Post-operation bleeding is one complication in any surgery. The dog had antibiotics and painkillers (tolfedine) and has no problem as evident by her normal behaviour and good appetite.
Toa Payoh Vets webpage
http://www.sinpets.com/F5/20111031old-dog-pterygium-glaucoma-anaesthetic-reactions-success-singapore-toapayohvets.htm
"Any bleeding from the eye?" I asked as there was some swelling of the stitched eye socket 3 hours after removal of the eyeball. In this case, I had stitched the conjunctival (upper and lower) tissues with 2/0 absorbable. Then I stitched the eyelid margins (as shown in the picture) with 3/0 nylon. So, there were two layers to prevent bleeding out of the eye.

"Some bleeding on the first day, but nothing serious. My dog is eating. I will see you 14 days later to remove the stitches."
Post-operation bleeding is one complication in any surgery. The dog had antibiotics and painkillers (tolfedine) and has no problem as evident by her normal behaviour and good appetite.
Toa Payoh Vets webpage
http://www.sinpets.com/F5/20111031old-dog-pterygium-glaucoma-anaesthetic-reactions-success-singapore-toapayohvets.htm
Monday, October 24, 2011
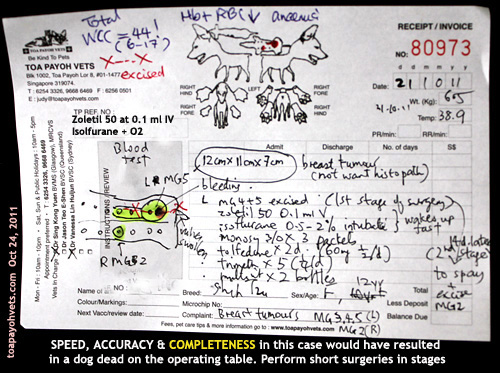
703. An old dog with a breast tumour bigger than 2 golf balls
"I went to Vet 1 as my dog was bleeding," the lady was concerned about the bleeding in her 12-year-old Shih Tzu rather than the tumours. "The vet bandaged the lump."
"Your dog has at least 4 breast tumours," I said. "How long did the biggest tumour take to grow?"
"Very fast," she said. "In the last month, it just grows so big." The tumour was the size of two golf balls. This was the left MG5 (the left caudal mammary gland, 5th gland)
HOW THIS CASE WAS HANDLED BY ME & DR VANESSA
1. Blood test compulsory.
Total white cell count was over 42 indicating a bacterial infection. I had the dog on IV drip and baytril overnight. Some owners object to blood tests due to financial considerations. X-ray of the chest would be preferred too but this is often not asked of the owner so as to reduce costs.
2. Surgery
Operation to be done the next day due to economic reasons. I prefer wait one week on antibiotics but there are such cases where the owner does not want to wait. Sometimes it may be better to reject such cases but compassion and the interest of the sick dog must be considered by the operating vet.
3. Pre-surgery - Zoletil
No sedation preferred. Just use isoflurane gas + oxygen.
Zoletil 0.1 ml IV although Dr Vanessa would have used Domitor. Isoflurane gas + oxygen via mask and then intubation. "Zoletil is safer in old dogs," I said. "Few vets I know use it for small animal sedation."
4. Short surgery
Only the big tumour was excised. This already took around 45 minutes. If the vet attempted to excise all, a dead dog would be the result as old dogs are very high anaesthetic risks.
In a recent on-going court case of a death of a man in his 40s who had liposuction and fat transfer to his chest, the general practitioner (GP) taking 3.5 hours for lipo-suction and transfer of fat to the chest of a man who died, I believe that the whole process of IV anaesthesia (involving topping up) took too long and lead to death. However, there were numerous perforations of the internal organs.
From what I read:
a) The expert witness mentioned about over-sedation as a cause of death as the patient did not respond even though he had numerous internal punctures.
b) The GP doctor doing the liposuction said death was due to fat embolism.
c) The GP doctor doing the IV anaesthesia (Propofol sedation given to effect iv and oxygen, but no general anaesthesia) said that the patient was alive at the end of surgery but died around half an hour later. Therefore anaesthesia was not the cause of death.
d) The autopsy report said death was due to numerous perforations of the intestines and the liver.
e) The judge was exasperated as to why the time and dosages of Propofol had not been made available before the inquest. The info was said to be in the GP's hard disk during the inquest. The case is on-going.
5. Anaesthesia
I was in charge of anaesthesia. The maintenance dose was 0.5 to 1.5% isoflurane. Towards the end of 30 minutes, I showed my assistant Min that the tongue has become white at the edges despite just 1.5%. I reduced to 0.5%. Switched off at the 2nd last stitch. The dog moved a bit. But stitching was done and the dog woke up. This was good anaesthesia. No delay in waking up and no need to use Antisedan as in the case of domitor.
6. Speed of surgery
6.1 Know your anatomy. There is the big blood vessel at around MG3 and MG4. Slow dissection and undermining is OK if you have time but old dog surgery need to be completed in less than 30 minutes for good anaesthetic outcome.
6.2 "No point having a perfect stitching and surgery if the dog dies on the operating table," I said to Dr Vanessa who started stitching up from one end intending to stitch at 0.5 cm intervals as this was her usual method. The wound was around 20 cm long. "Stitch at 1 cm intervals." I also advised stitching at the major points first e.g place 4 stitches and then continue stitching in between.
6.3 "Use walk-in sutures," I explained. But Dr Vanessa was comfortable in using subcuticular sutures to hold the subcutaneous fat together. This took much more time as skin sutures were then sutured with simple interrupted sutures. In "walk-in sutures," I would stitch the skin, then subcutaneous fat and then skin all in one movement using horizontal mattress sutures on the skin.
OUTCOME
The whole process was completed by Dr Vanessa in around 45 minutes. Any longer would have caused death, in my opinion as the tongue was turning pale pinkish cyantotic and white at the edges.
The dog was alive and that was what the owner expected. She had come in the morning of the surgery on Day 2 to ask more questions. I had to be frank as I told her that I needed time to prepare for surgery.
In the evening the happy owner took the dog home. I write this case as a mentoring case done by me.
QUESTIONS ASKED
1. The financial considerations which were addressed yesterday.
2. The chances of survival. Hard to predict as the dog had a bacterial infection and was old at 12 years. Short surgeries make survival likely. So, the other tumours and spaying of the dog had been advised for two weeks later.
3. Whether the breast tumour is cancerous. Most likely as it grows explosively big within a month.
4. Will the tumour come back? Most likely as it is cancerous. However, the owner does not want histopathology by the lab to confirm it.
CONCLUSION
No matter how great the vet surgeon is, anaesthesia is the most important in any surgery as a dog alive is what the owner wants. Beautiful surgery is a bonus.
Toa Payoh Vets webpage is at:
http://www.sinpets.com/F6/20111035old-dog-zoletil-breast-tumours-singapore-toapayohvets.htm
"Your dog has at least 4 breast tumours," I said. "How long did the biggest tumour take to grow?"
"Very fast," she said. "In the last month, it just grows so big." The tumour was the size of two golf balls. This was the left MG5 (the left caudal mammary gland, 5th gland)
HOW THIS CASE WAS HANDLED BY ME & DR VANESSA
1. Blood test compulsory.
Total white cell count was over 42 indicating a bacterial infection. I had the dog on IV drip and baytril overnight. Some owners object to blood tests due to financial considerations. X-ray of the chest would be preferred too but this is often not asked of the owner so as to reduce costs.
2. Surgery
Operation to be done the next day due to economic reasons. I prefer wait one week on antibiotics but there are such cases where the owner does not want to wait. Sometimes it may be better to reject such cases but compassion and the interest of the sick dog must be considered by the operating vet.
3. Pre-surgery - Zoletil
No sedation preferred. Just use isoflurane gas + oxygen.
Zoletil 0.1 ml IV although Dr Vanessa would have used Domitor. Isoflurane gas + oxygen via mask and then intubation. "Zoletil is safer in old dogs," I said. "Few vets I know use it for small animal sedation."
4. Short surgery
Only the big tumour was excised. This already took around 45 minutes. If the vet attempted to excise all, a dead dog would be the result as old dogs are very high anaesthetic risks.
In a recent on-going court case of a death of a man in his 40s who had liposuction and fat transfer to his chest, the general practitioner (GP) taking 3.5 hours for lipo-suction and transfer of fat to the chest of a man who died, I believe that the whole process of IV anaesthesia (involving topping up) took too long and lead to death. However, there were numerous perforations of the internal organs.
From what I read:
a) The expert witness mentioned about over-sedation as a cause of death as the patient did not respond even though he had numerous internal punctures.
b) The GP doctor doing the liposuction said death was due to fat embolism.
c) The GP doctor doing the IV anaesthesia (Propofol sedation given to effect iv and oxygen, but no general anaesthesia) said that the patient was alive at the end of surgery but died around half an hour later. Therefore anaesthesia was not the cause of death.
d) The autopsy report said death was due to numerous perforations of the intestines and the liver.
e) The judge was exasperated as to why the time and dosages of Propofol had not been made available before the inquest. The info was said to be in the GP's hard disk during the inquest. The case is on-going.
5. Anaesthesia
I was in charge of anaesthesia. The maintenance dose was 0.5 to 1.5% isoflurane. Towards the end of 30 minutes, I showed my assistant Min that the tongue has become white at the edges despite just 1.5%. I reduced to 0.5%. Switched off at the 2nd last stitch. The dog moved a bit. But stitching was done and the dog woke up. This was good anaesthesia. No delay in waking up and no need to use Antisedan as in the case of domitor.
6. Speed of surgery
6.1 Know your anatomy. There is the big blood vessel at around MG3 and MG4. Slow dissection and undermining is OK if you have time but old dog surgery need to be completed in less than 30 minutes for good anaesthetic outcome.
6.2 "No point having a perfect stitching and surgery if the dog dies on the operating table," I said to Dr Vanessa who started stitching up from one end intending to stitch at 0.5 cm intervals as this was her usual method. The wound was around 20 cm long. "Stitch at 1 cm intervals." I also advised stitching at the major points first e.g place 4 stitches and then continue stitching in between.
6.3 "Use walk-in sutures," I explained. But Dr Vanessa was comfortable in using subcuticular sutures to hold the subcutaneous fat together. This took much more time as skin sutures were then sutured with simple interrupted sutures. In "walk-in sutures," I would stitch the skin, then subcutaneous fat and then skin all in one movement using horizontal mattress sutures on the skin.
OUTCOME
The whole process was completed by Dr Vanessa in around 45 minutes. Any longer would have caused death, in my opinion as the tongue was turning pale pinkish cyantotic and white at the edges.
The dog was alive and that was what the owner expected. She had come in the morning of the surgery on Day 2 to ask more questions. I had to be frank as I told her that I needed time to prepare for surgery.
In the evening the happy owner took the dog home. I write this case as a mentoring case done by me.
QUESTIONS ASKED
1. The financial considerations which were addressed yesterday.
2. The chances of survival. Hard to predict as the dog had a bacterial infection and was old at 12 years. Short surgeries make survival likely. So, the other tumours and spaying of the dog had been advised for two weeks later.
3. Whether the breast tumour is cancerous. Most likely as it grows explosively big within a month.
4. Will the tumour come back? Most likely as it is cancerous. However, the owner does not want histopathology by the lab to confirm it.
CONCLUSION
No matter how great the vet surgeon is, anaesthesia is the most important in any surgery as a dog alive is what the owner wants. Beautiful surgery is a bonus.
Toa Payoh Vets webpage is at:
http://www.sinpets.com/F6/20111035old-dog-zoletil-breast-tumours-singapore-toapayohvets.htm
Sunday, October 23, 2011
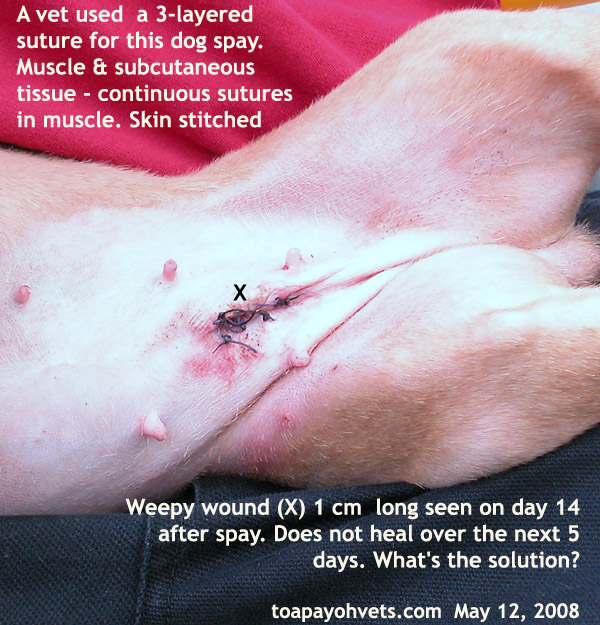
Keep Spay Surgery Simple - No subcuticular suturing
I am writing to share my over 30 years of experiences in spaying dogs and cats done by me and by other vets in Toa Payoh Vets.
I started Toa Payoh Vets in 1982 and it is 2011 now. I have seen a few cases of stitch breakdown using the method as advised by the university professors and veterinary surgery text books (Method 1).
The vet university professors since my time in 1974 when I graduated from Glasgow University and even recently in Australian Universities, advocate the following steps after removing the ovaries and uterus:
1. suture the linea alba
2. suture the subcutaneous fat to seal up dead spaces
3. suture the skin
The theory is sound and many newly graduated vets adopt this system (Method 1). Over the years, I encountered a few cases of stitch breakdown and infection in dogs and cats using Method 1 done by other vets. Or intense redness and inflammation at the surgical area.
My method does NOT use Step 2 and I have less than 1% of post-op stitch breakdown. I have no figures to substantiate my claim. I am merely sharing my experiences as I am in my retirement era, being 61 years of age.
I just hope that this knowledge may benefit the dogs and cats. In the early years of 1970 - 1980, I did not prescribe pain-killers unlike nowadays and I don't have many post-op spay problems. Times have changed. Pain-killers inclusive of antibiotics are a must.
There are many reasons for stitch breakdown but one of them is the irritating subcutaneous suture. The dog or cat keeps licking the wound or just use the hind paws to scratch it. E-collars do not help much. Soon, the unhappy owner brings in the dog or cat for review.
In private practice, the vet earns his reputation by not getting less or no post-op spay stitch breakdown as owners will compare and complain. Obviously, in other surgery like breast tumour removal, subcuticular sutures are needed to close the dead spaces. I use "walk-in" sutures. This involves suture needle going into the skin, then into the subcutaneous fat and out of the subcutaneous fat, then out of the skin on the other side. From there, I transverse, needle goes into the skin, subcutaneous fat and out from the initial side. This makes for a horizontal mattress skin suture as seen from the skin. In this method, surgical time is reduced, unlike separate subcuticular sutures of the subcutaneous fat. See case report at:
http://www.bekindtopets.com/dogs/20081235Mastectomy_Female_Dog_ToaPayohVets.htm
Then simple interrupted sutures of the skin as this is a usual method by many vets.
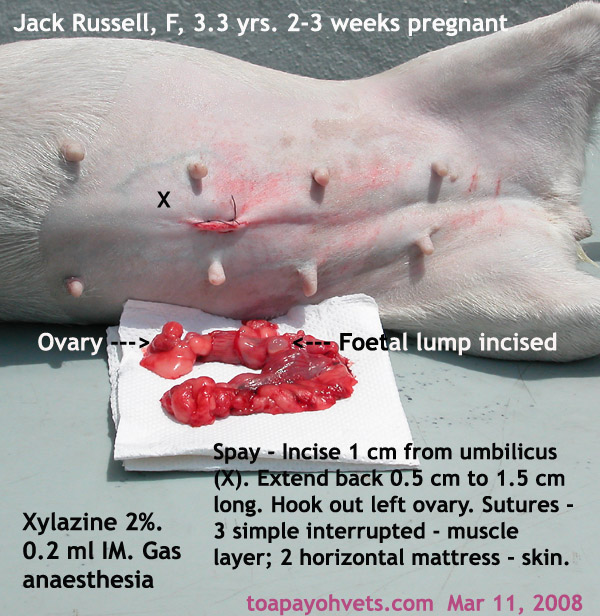
The two methods of SPAY IN THE DOG AND CAT are illustrated by real cases as follows:
METHOD 1 - BY THE (VETERINARY SURGERY) BOOK

1298. Subcuticular sutures have been used. The stitches under the skin hinder healing due to infections or traumatic injury from licking.
1299. Stitch breakdown and infection. Re-stitch again but no more subcuticular suturing.
METHOD 2 - BY DR SING

1296. A spay hook enables the vet to make spay incision small in the dog and cat.
1297. Dr Sing's dog spay procedures. No subcuticular sutures.
All the years, I use absorbable PDS sutures and this means the owner does NOT need to return for stitch removal. I just use one packet of sutures. However, with Method 1, I note that some of the younger vets must use two packets and sometimes three packets in dogs that are pregnant and of bigger breeds.
I have seen cases where a vet uses 3 packets of sutures to spay a medium sized dog. This is definitely too many. One packet is chromic catgut. Two packets of absorbable monofilament. With my method, one packet of absorbable suture is sufficient for dogs up to medium size, using the spay hook.
Keep spay simple. I hope this report is of use to some practising vets. It cuts down on expenses in using more sutures and in private practice, costs keep rising as bureaucrats think of ways and means to generate income from the industry by increasing regulatory fees. Keeping spay simple and using walk-in sutures make economic sense as well as keep owners of dogs and cats happier.
OTHER INFORMATION
4448. KPI - How long it takes to spay a female dog? 26 or 18 minutes?
4451. Surgery Audit: How long it takes to spay a female dog? 18 minutes
4438 - 4444. When do you remove the dressing or stitches after spay/neuter?
4475. Never discharge a spayed dog with a hole in the operation area
Toa Payoh Vets webpage is at:
http://www.sinpets.com/F6/20111033spay-cat-dog-no-subcuticular-singapore-toapayohvets.htm
I started Toa Payoh Vets in 1982 and it is 2011 now. I have seen a few cases of stitch breakdown using the method as advised by the university professors and veterinary surgery text books (Method 1).
The vet university professors since my time in 1974 when I graduated from Glasgow University and even recently in Australian Universities, advocate the following steps after removing the ovaries and uterus:
1. suture the linea alba
2. suture the subcutaneous fat to seal up dead spaces
3. suture the skin
The theory is sound and many newly graduated vets adopt this system (Method 1). Over the years, I encountered a few cases of stitch breakdown and infection in dogs and cats using Method 1 done by other vets. Or intense redness and inflammation at the surgical area.
My method does NOT use Step 2 and I have less than 1% of post-op stitch breakdown. I have no figures to substantiate my claim. I am merely sharing my experiences as I am in my retirement era, being 61 years of age.
I just hope that this knowledge may benefit the dogs and cats. In the early years of 1970 - 1980, I did not prescribe pain-killers unlike nowadays and I don't have many post-op spay problems. Times have changed. Pain-killers inclusive of antibiotics are a must.
There are many reasons for stitch breakdown but one of them is the irritating subcutaneous suture. The dog or cat keeps licking the wound or just use the hind paws to scratch it. E-collars do not help much. Soon, the unhappy owner brings in the dog or cat for review.
In private practice, the vet earns his reputation by not getting less or no post-op spay stitch breakdown as owners will compare and complain. Obviously, in other surgery like breast tumour removal, subcuticular sutures are needed to close the dead spaces. I use "walk-in" sutures. This involves suture needle going into the skin, then into the subcutaneous fat and out of the subcutaneous fat, then out of the skin on the other side. From there, I transverse, needle goes into the skin, subcutaneous fat and out from the initial side. This makes for a horizontal mattress skin suture as seen from the skin. In this method, surgical time is reduced, unlike separate subcuticular sutures of the subcutaneous fat. See case report at:
http://www.bekindtopets.com/dogs/20081235Mastectomy_Female_Dog_ToaPayohVets.htm
Then simple interrupted sutures of the skin as this is a usual method by many vets.
The two methods of SPAY IN THE DOG AND CAT are illustrated by real cases as follows:
METHOD 1 - BY THE (VETERINARY SURGERY) BOOK
1298. Subcuticular sutures have been used. The stitches under the skin hinder healing due to infections or traumatic injury from licking.
1299. Stitch breakdown and infection. Re-stitch again but no more subcuticular suturing.
METHOD 2 - BY DR SING
1296. A spay hook enables the vet to make spay incision small in the dog and cat.
1297. Dr Sing's dog spay procedures. No subcuticular sutures.
All the years, I use absorbable PDS sutures and this means the owner does NOT need to return for stitch removal. I just use one packet of sutures. However, with Method 1, I note that some of the younger vets must use two packets and sometimes three packets in dogs that are pregnant and of bigger breeds.
I have seen cases where a vet uses 3 packets of sutures to spay a medium sized dog. This is definitely too many. One packet is chromic catgut. Two packets of absorbable monofilament. With my method, one packet of absorbable suture is sufficient for dogs up to medium size, using the spay hook.
Keep spay simple. I hope this report is of use to some practising vets. It cuts down on expenses in using more sutures and in private practice, costs keep rising as bureaucrats think of ways and means to generate income from the industry by increasing regulatory fees. Keeping spay simple and using walk-in sutures make economic sense as well as keep owners of dogs and cats happier.
OTHER INFORMATION
4448. KPI - How long it takes to spay a female dog? 26 or 18 minutes?
4451. Surgery Audit: How long it takes to spay a female dog? 18 minutes
4438 - 4444. When do you remove the dressing or stitches after spay/neuter?
4475. Never discharge a spayed dog with a hole in the operation area
Toa Payoh Vets webpage is at:
http://www.sinpets.com/F6/20111033spay-cat-dog-no-subcuticular-singapore-toapayohvets.htm
701. Follow up on: Pterygium + Glaucoma + Haematoma in 2010, Enucleation in 2011
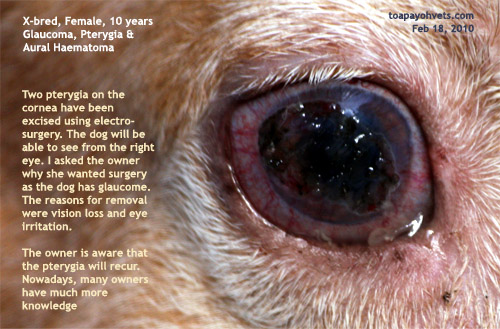
What is a pterygium? It is an invasive proliferative fibrovascular growth.
Excision of the pterygia was requested by the owner as the dog had difficulty seeing in the right eye and kept rubbing the right eye.
Excision was by electro-surgery under general anaesthesia. In human medicine, there are various sophisticated surgical methods used
I find that many old dogs can survive if the surgery and anaesthesia can be done under 15 minutes. Provided there is care in the anaesthesia and knowledge of emergency resuscitation. The anaesthetic time would be prolonged as there were two pterygia to be excised.
The Divine Powers above threw in an ear haematoma to be operated too. That meant a much longer anaesthetic time.
The longer the anaesthesia, the higher the chances of the old dog dying on the operating table.
This dog needed over 60 minutes of surgery. Would his cornea rupture? That would increase the anaesthetic time.
The dog did not wake up within 2 minutes at the end of anaesthesia.
An antidote (Antisedan) woke him up. He recovered smoothly on Domitor pre-anaesthetic dose, isoflurane gas maintenance and Antisedan anti-dote. He woke up quietly as if he had a good nap.
Fortunately, the mission was accomplished with excellent anaesthesia. This story had a happy ending for everyone. Further info is as follows:
In March 20, 2003, I saw a Shih Tzu puppy with a growth on the right eye for the first time. Was this a rare case of a pterygium? No. It was a Dermoid as it had hairs and was of a different colour. See: Mar 20 03. The Shih Tzu puppy has a "pterygium"?
7 years had passed since I saw the afore-mentioned Shih Tzu puppy with the Dermoid. A real case of pterygium surfaced in February 2010.
She was more knowledgeable than me in specific area affecting this very gentle X-bred dog, as she correctly stated: "My dog has a pterygium," when she first consulted me. She requested me to excise the two bulging growths on the cornea of her dog.
The dog also had glaucoma. She was old. There was a big risk that the cornea might rupture. The bigger risk was death on the operating table as this old dog would be a high anaesthetic risk. Every old dog under anaesthesia is a big risk and deaths from anaesthesia are very unpleasant for the vet as the whole family never forgets nor forgives when the outcome is a dead body. I was very apprehensive that this well cared for and loved family member would die on the operating table as anaesthesia would take a long time to excise two pterygia. As if my worries were not sufficient, the dog also had a right ear haematoma to be operated upon. That meant that the surgery would take over an hour!
The longer the operation, the higher the chances of deaths on the operating table.
"Why do you want the pterygia removed?" I asked the determined owner.
"My dog walked towards her left when the pterygia started to grow fast towards the centre of the cornea. She cannot see from her right eye as the pterygium had obstructed her vision." the owner said. "In addition, she keeps scratching her right eye."
"If the cornea ruptures during excision, I will have to remove the whole eyeball," I said. "Yes," the lady consented. There was this understanding and awareness of the high risk of the cornea bursting when I excise the pterygium when the intraocular pressure was very high. One pterygium was already worrisome. But this dog had two big ones.
"Have you considered enucleation (eyeball removal)?" I asked as glaucoma can be a very painful condition and treatment using eye drops must be given regularly and drug control may become ineffective over time. I don't know much about its glaucoma formation as it was treated by another vet. Glaucoma was controlled by eye drops.
"The other vet has recommended it," she said. "But my family does not want the dog to lose his eye." So enucleation was out of question.
As to what caused such a rapid growth of the pterygia in this beloved dog, it is hard to say. In people, pterygium is said to be caused by ultra-violet light exposure.
It was fortunate that the old dog survived the anaesthesia and went home. "Take good care of her glaucoma," I said to the happy lady as I discovered that the old e-collar was no more worn. I had asked whether she still had the e-collar and she said it was worn out and disposed. "That means that she must wear the e-collar all the time for many weeks and stay out of the sunlight and wind." 7 days later, I would need to review this case.
Pterygia Surgery at Toa Payoh Vets


Haematoma Surgery At Toa Payoh Vets
Toa Payoh Vets webpage and images for this article is:
http://www.sinpets.com/F6/20111023pterygia-glaucoma-haematoma-dog-toapayohvets-singapore.htm
FOLLOW UP IN 2011
In 2011, the dog's eye was enucleated. The webpage at Toa Payoh Vets is at:
http://www.sinpets.com/F5/20111031old-dog-pterygium-glaucoma-anaesthetic-reactions-success-singapore-toapayohvets.htm

Excision of the pterygia was requested by the owner as the dog had difficulty seeing in the right eye and kept rubbing the right eye.
Excision was by electro-surgery under general anaesthesia. In human medicine, there are various sophisticated surgical methods used
I find that many old dogs can survive if the surgery and anaesthesia can be done under 15 minutes. Provided there is care in the anaesthesia and knowledge of emergency resuscitation. The anaesthetic time would be prolonged as there were two pterygia to be excised.
The Divine Powers above threw in an ear haematoma to be operated too. That meant a much longer anaesthetic time.
The longer the anaesthesia, the higher the chances of the old dog dying on the operating table.
This dog needed over 60 minutes of surgery. Would his cornea rupture? That would increase the anaesthetic time.
The dog did not wake up within 2 minutes at the end of anaesthesia.
An antidote (Antisedan) woke him up. He recovered smoothly on Domitor pre-anaesthetic dose, isoflurane gas maintenance and Antisedan anti-dote. He woke up quietly as if he had a good nap.
Fortunately, the mission was accomplished with excellent anaesthesia. This story had a happy ending for everyone. Further info is as follows:
In March 20, 2003, I saw a Shih Tzu puppy with a growth on the right eye for the first time. Was this a rare case of a pterygium? No. It was a Dermoid as it had hairs and was of a different colour. See: Mar 20 03. The Shih Tzu puppy has a "pterygium"?
7 years had passed since I saw the afore-mentioned Shih Tzu puppy with the Dermoid. A real case of pterygium surfaced in February 2010.
She was more knowledgeable than me in specific area affecting this very gentle X-bred dog, as she correctly stated: "My dog has a pterygium," when she first consulted me. She requested me to excise the two bulging growths on the cornea of her dog.
The dog also had glaucoma. She was old. There was a big risk that the cornea might rupture. The bigger risk was death on the operating table as this old dog would be a high anaesthetic risk. Every old dog under anaesthesia is a big risk and deaths from anaesthesia are very unpleasant for the vet as the whole family never forgets nor forgives when the outcome is a dead body. I was very apprehensive that this well cared for and loved family member would die on the operating table as anaesthesia would take a long time to excise two pterygia. As if my worries were not sufficient, the dog also had a right ear haematoma to be operated upon. That meant that the surgery would take over an hour!
The longer the operation, the higher the chances of deaths on the operating table.
"Why do you want the pterygia removed?" I asked the determined owner.
"My dog walked towards her left when the pterygia started to grow fast towards the centre of the cornea. She cannot see from her right eye as the pterygium had obstructed her vision." the owner said. "In addition, she keeps scratching her right eye."
"If the cornea ruptures during excision, I will have to remove the whole eyeball," I said. "Yes," the lady consented. There was this understanding and awareness of the high risk of the cornea bursting when I excise the pterygium when the intraocular pressure was very high. One pterygium was already worrisome. But this dog had two big ones.
"Have you considered enucleation (eyeball removal)?" I asked as glaucoma can be a very painful condition and treatment using eye drops must be given regularly and drug control may become ineffective over time. I don't know much about its glaucoma formation as it was treated by another vet. Glaucoma was controlled by eye drops.
"The other vet has recommended it," she said. "But my family does not want the dog to lose his eye." So enucleation was out of question.
As to what caused such a rapid growth of the pterygia in this beloved dog, it is hard to say. In people, pterygium is said to be caused by ultra-violet light exposure.
It was fortunate that the old dog survived the anaesthesia and went home. "Take good care of her glaucoma," I said to the happy lady as I discovered that the old e-collar was no more worn. I had asked whether she still had the e-collar and she said it was worn out and disposed. "That means that she must wear the e-collar all the time for many weeks and stay out of the sunlight and wind." 7 days later, I would need to review this case.
Pterygia Surgery at Toa Payoh Vets

Haematoma Surgery At Toa Payoh Vets
Toa Payoh Vets webpage and images for this article is:
http://www.sinpets.com/F6/20111023pterygia-glaucoma-haematoma-dog-toapayohvets-singapore.htm
FOLLOW UP IN 2011
In 2011, the dog's eye was enucleated. The webpage at Toa Payoh Vets is at:
http://www.sinpets.com/F5/20111031old-dog-pterygium-glaucoma-anaesthetic-reactions-success-singapore-toapayohvets.htm

Friday, October 21, 2011
700. Follow up on paper training and stool eating puppy
LATEST E-MAIL REPLY FROM DR SING DATED OCT 21, 2011
Paper shredding is a common complaint in paper-training. Taping the edges is one method which you have used successfully.
Stool eating is a difficult problem to solve as the cause is usually unknown.
1. Pepper, chilli sauce and others have been added onto the stools without effect.
2. Some owners buy the "anti-stool" eating powder from the pet shops and claim effectiveness as long as the powder is eaten.
3. Others add pineapple slices onto the food and claim good results.
4. Distraction methods: Another writer advise putting a can of coins on top of the door. Hide somewhere. When the puppy eats the stools, the can of coins drop onto the floor. Personally I doubt that the puppy (as a canine with sensitive hearing) will not know that the owner is hiding somewhere.
5. Another method is to squirt water onto the puppy when he eats his stools. You need a water gun.
6. As you can see, it is extremely difficult to resolve the problem. Picking up the stools immediately (without making a fuss) seem to be another method. In this way, it is hoped that the puppy outgrows this bad habit. Otherwise he continues the habit to old age. This appears to be what you are doing.
7. My idea is to take the puppy outdoors to poop after meals but this may not be practical for you if you live in a high rise. This involves a routine as follows: Puppy completed eating. Take him outdoors to the grass. In short, take the puppy to another area (e.g. balcony has newspapers with smell of poop) to poop. This works if the puppy poops within 10 minutes after eating and the owner is free to do this consistently for 2-4 weeks.
----------------------------------------------------------------------------
On Thu, Oct 20, 2011 at 9:50 PM, A@gmail.com> wrote:
Hi Dr Sing,
I hope this email finds you well.
It has been almost a week since we tried your suggestion. Newspapers (full page, spread out) are placed on the top right corner of the toilet and the puppy eliminates at the area. We are slowly trying to reduce the area of the newspaper. Attached is a picture of the toilet for your reference.
 However, he has started to (in this order, not sure if it tells you anything) smell, lick and eat his stools. Soiled papers are changed almost immediately in the day, as someone is usually around to hear him running on the newspapers. One of us will wake up in the middle of the night every few hours to check on him and clear any waste, but sometimes he has already finished eating his stools. We are cautious not to disturb him when he eliminates. Pepper does not help as he eats his stools which has pepper. Is there anything we can do about this?
However, he has started to (in this order, not sure if it tells you anything) smell, lick and eat his stools. Soiled papers are changed almost immediately in the day, as someone is usually around to hear him running on the newspapers. One of us will wake up in the middle of the night every few hours to check on him and clear any waste, but sometimes he has already finished eating his stools. We are cautious not to disturb him when he eliminates. Pepper does not help as he eats his stools which has pepper. Is there anything we can do about this?
As the puppy loves to shred newspapers, we use masking tape and lace it white vinegar to prevent him from peeling off the tape. It works most of the time, and he does his business as usual, including eating his poop.
Once again, thanks for your advise and I hope to hear from you soon.
Best regards,
A
------------------------------------------------------------------
From: A
Sent: Friday, October 14, 2011 10:00 PM
To: Kong Yuen Sing
Subject: Re: paper training problems for a 3 month old poodle
Hi Dr Sing,
Appreciate your prompt reply, we are currently trying it out and will let you know how it goes. Have a nice weekend. :)
Best regards,
A
--------------------------------------------------------------------------
From: Kong Yuen Sing
Sent: Friday, October 14, 2011 7:04 AM
To: A
Subject: Re: paper training problems for a 3 month old poodle
Thank you for your detailed e-mail and the 3 images. As every puppy and owner is different in personality and training experience, the following reply may or may not be useful to you.
1. You have confused the puppy in attempting to grate-train (using the cage) and paper-train him (inside the at the same time. Puppies, like babies, are creatures of routine. One method of toilet training is needed. Either grate-training or paper training.
2. At the pet shop, the puppy has had been trained to eliminate in the grate (floor of the crate or cage). This type of grate+pee pan housing is prevalent in the Singapore pet shops as shown in the image you posted to me. The puppy wanted to eliminate on the grate but you wanted him to do on the paper and most likely paid extra attention and fuss. So, the puppy was not free to eliminate in privacy after eating as in the pet shop.
3. To make a long story short, I would propose just write about paper training as I presume this is what you want to achieve instead of writing about grate+pee pan training or both methods. The grate+pee pan method involves buying the grate + pee pan separately or the use of your existing crate.
PAPER TRAINING
3.1 You confine the puppy inside the toilet. Install a baby-gate. Cover the toilet floor 100% with paper. At one corner (e.g. left half, back), away from the baby gate, put a piece of paper with the puppy's urine or tissue paper with his urine smell. At the other corner (e.g. right half, front), his food and water. In the right half, place his towel, bed, or floor mat, for example. This will be his clean area.
3.2 The puppy is left there for the next 2 - 4 weeks and given privacy, not stressed out by your scoldings or presence or the presence of children and family members during eating for at least 1 hour.
3.3 The puppy can be taken out to play after he has pooped regularly and this may take a week. This is where you observe signs of elimination (squatting, turning) and put him quickly back to his toilet.
3.4 Change soiled papers frequently.
3.5 Within 7 days, you should see that the papered corner where the puppy pees and poops will be. Reduce the paper area.
3.6 If the puppy shreds the paper, you still need to persevere and do not scold or shout at him.
In conclusion, confinement for the first 2-4 weeks is the key to success in toilet training. What you do during the confinement will require your perseverance, hard work of keeping the puppy's "den" (toilet) clean.
The training is much more than what I write. The devil is in the execution. Pl let me know when you have succeeded or if you have more queries.
Best wishes.
-------------------------------------------------------------------------------
On Thu, Oct 13, 2011 at 9:34 PM, .........@gmail.com> wrote:
Dear Dr Sing,
I would like to seek your advise with regards to paper training. Three pictures are attached for your reference; a picture of the cage he sleeps in, the toilet area with newspaper, and a view of his cage from the toilet.
I have a 3 month old male miniature poodle whom I brought home about a week ago from a pet shop. We bought him a cage and are in the process of training him to eliminate in the toilet on the newspaper. At the pet shop, he would eliminate about 15 minutes after his meal. However, he eliminates only after a few hours. For example, we will give him dinner at 7.30PM and most of the time he will not eliminate until the next morning. It is rare that he will eliminate within 2 hours. When we spot signs that he wants to eliminate when he is outside the cage, we will bring him to the toilet and coax him to eliminate, whether big or small ‘business’. Most of the time he will not do it unless he has not gone into his cage for a very long time, say a few hours. There are times when he will run to the toilet and smell the newspapers, only to run out, which we take as a hint that he wants to eliminate and put him into the toilet telling him to pee, using the same word every time. Rewards given when he does the right thing.
When we put him into the cage, he will eliminate within a few minutes or even seconds when we are not looking, and that is after we have just brought him to the toilet. The areas which he eliminates in the cage are not consistent. Even if he does not intend to eliminate, he will turn in circles and give us false alarms, as I believe he knows we will bring him out when he does that. We tried washing his entire cage with antiseptic but he still does it inside the cage. The newspapers in the toilet have traces of his pee and also a kind of liquid we bought from the pet shop to help him recognise the place.
For the first two or three days, he used to pee all over the place but after scolding him a few times and cleaning with vinegar, he has not done it since. A crate didn’t help as he peed inside it.
Are we doing something wrong? Some expressed their opinion that a pee tray would be better and the distance between the toilet and cage is too far for him, making him confused. He has not had his third vaccination so we have yet to bring him out.
Thank you very much for taking time to read this email, and also for your informative articles. Looking forward to hear from you soon!
Best regards,
Name
DETAILS AT TOA PAYOH VETS
http://www.sinpets.com/F5/20111023puppy-toilet-training-paper-or-grate-not-both-singapore-toapayohvets.htm
Paper shredding is a common complaint in paper-training. Taping the edges is one method which you have used successfully.
Stool eating is a difficult problem to solve as the cause is usually unknown.
1. Pepper, chilli sauce and others have been added onto the stools without effect.
2. Some owners buy the "anti-stool" eating powder from the pet shops and claim effectiveness as long as the powder is eaten.
3. Others add pineapple slices onto the food and claim good results.
4. Distraction methods: Another writer advise putting a can of coins on top of the door. Hide somewhere. When the puppy eats the stools, the can of coins drop onto the floor. Personally I doubt that the puppy (as a canine with sensitive hearing) will not know that the owner is hiding somewhere.
5. Another method is to squirt water onto the puppy when he eats his stools. You need a water gun.
6. As you can see, it is extremely difficult to resolve the problem. Picking up the stools immediately (without making a fuss) seem to be another method. In this way, it is hoped that the puppy outgrows this bad habit. Otherwise he continues the habit to old age. This appears to be what you are doing.
7. My idea is to take the puppy outdoors to poop after meals but this may not be practical for you if you live in a high rise. This involves a routine as follows: Puppy completed eating. Take him outdoors to the grass. In short, take the puppy to another area (e.g. balcony has newspapers with smell of poop) to poop. This works if the puppy poops within 10 minutes after eating and the owner is free to do this consistently for 2-4 weeks.
----------------------------------------------------------------------------
On Thu, Oct 20, 2011 at 9:50 PM, A@gmail.com> wrote:
Hi Dr Sing,
I hope this email finds you well.
It has been almost a week since we tried your suggestion. Newspapers (full page, spread out) are placed on the top right corner of the toilet and the puppy eliminates at the area. We are slowly trying to reduce the area of the newspaper. Attached is a picture of the toilet for your reference.

As the puppy loves to shred newspapers, we use masking tape and lace it white vinegar to prevent him from peeling off the tape. It works most of the time, and he does his business as usual, including eating his poop.
Once again, thanks for your advise and I hope to hear from you soon.
Best regards,
A
------------------------------------------------------------------
From: A
Sent: Friday, October 14, 2011 10:00 PM
To: Kong Yuen Sing
Subject: Re: paper training problems for a 3 month old poodle
Hi Dr Sing,
Appreciate your prompt reply, we are currently trying it out and will let you know how it goes. Have a nice weekend. :)
Best regards,
A
--------------------------------------------------------------------------
From: Kong Yuen Sing
Sent: Friday, October 14, 2011 7:04 AM
To: A
Subject: Re: paper training problems for a 3 month old poodle
Thank you for your detailed e-mail and the 3 images. As every puppy and owner is different in personality and training experience, the following reply may or may not be useful to you.
1. You have confused the puppy in attempting to grate-train (using the cage) and paper-train him (inside the at the same time. Puppies, like babies, are creatures of routine. One method of toilet training is needed. Either grate-training or paper training.
2. At the pet shop, the puppy has had been trained to eliminate in the grate (floor of the crate or cage). This type of grate+pee pan housing is prevalent in the Singapore pet shops as shown in the image you posted to me. The puppy wanted to eliminate on the grate but you wanted him to do on the paper and most likely paid extra attention and fuss. So, the puppy was not free to eliminate in privacy after eating as in the pet shop.
3. To make a long story short, I would propose just write about paper training as I presume this is what you want to achieve instead of writing about grate+pee pan training or both methods. The grate+pee pan method involves buying the grate + pee pan separately or the use of your existing crate.
PAPER TRAINING
3.1 You confine the puppy inside the toilet. Install a baby-gate. Cover the toilet floor 100% with paper. At one corner (e.g. left half, back), away from the baby gate, put a piece of paper with the puppy's urine or tissue paper with his urine smell. At the other corner (e.g. right half, front), his food and water. In the right half, place his towel, bed, or floor mat, for example. This will be his clean area.
3.2 The puppy is left there for the next 2 - 4 weeks and given privacy, not stressed out by your scoldings or presence or the presence of children and family members during eating for at least 1 hour.
3.3 The puppy can be taken out to play after he has pooped regularly and this may take a week. This is where you observe signs of elimination (squatting, turning) and put him quickly back to his toilet.
3.4 Change soiled papers frequently.
3.5 Within 7 days, you should see that the papered corner where the puppy pees and poops will be. Reduce the paper area.
3.6 If the puppy shreds the paper, you still need to persevere and do not scold or shout at him.
In conclusion, confinement for the first 2-4 weeks is the key to success in toilet training. What you do during the confinement will require your perseverance, hard work of keeping the puppy's "den" (toilet) clean.
The training is much more than what I write. The devil is in the execution. Pl let me know when you have succeeded or if you have more queries.
Best wishes.
-------------------------------------------------------------------------------
On Thu, Oct 13, 2011 at 9:34 PM, .........@gmail.com> wrote:
Dear Dr Sing,
I would like to seek your advise with regards to paper training. Three pictures are attached for your reference; a picture of the cage he sleeps in, the toilet area with newspaper, and a view of his cage from the toilet.
I have a 3 month old male miniature poodle whom I brought home about a week ago from a pet shop. We bought him a cage and are in the process of training him to eliminate in the toilet on the newspaper. At the pet shop, he would eliminate about 15 minutes after his meal. However, he eliminates only after a few hours. For example, we will give him dinner at 7.30PM and most of the time he will not eliminate until the next morning. It is rare that he will eliminate within 2 hours. When we spot signs that he wants to eliminate when he is outside the cage, we will bring him to the toilet and coax him to eliminate, whether big or small ‘business’. Most of the time he will not do it unless he has not gone into his cage for a very long time, say a few hours. There are times when he will run to the toilet and smell the newspapers, only to run out, which we take as a hint that he wants to eliminate and put him into the toilet telling him to pee, using the same word every time. Rewards given when he does the right thing.
When we put him into the cage, he will eliminate within a few minutes or even seconds when we are not looking, and that is after we have just brought him to the toilet. The areas which he eliminates in the cage are not consistent. Even if he does not intend to eliminate, he will turn in circles and give us false alarms, as I believe he knows we will bring him out when he does that. We tried washing his entire cage with antiseptic but he still does it inside the cage. The newspapers in the toilet have traces of his pee and also a kind of liquid we bought from the pet shop to help him recognise the place.
For the first two or three days, he used to pee all over the place but after scolding him a few times and cleaning with vinegar, he has not done it since. A crate didn’t help as he peed inside it.
Are we doing something wrong? Some expressed their opinion that a pee tray would be better and the distance between the toilet and cage is too far for him, making him confused. He has not had his third vaccination so we have yet to bring him out.
Thank you very much for taking time to read this email, and also for your informative articles. Looking forward to hear from you soon!
Best regards,
Name
DETAILS AT TOA PAYOH VETS
http://www.sinpets.com/F5/20111023puppy-toilet-training-paper-or-grate-not-both-singapore-toapayohvets.htm
Thursday, October 20, 2011
699. Liposuction Death - Practice guidelines for safe sedation
Straits Times, oct 20, 2011 Pg A4
Liposuction Death - I did not cause death, says doctor
Patient: Mr Heng went to Reves Clinic in Orchard Rd on Dec 30, 2009 for a liposuction and fat-transfer operation.
Doctor 1: Dr Jim Wong did the surgery. Set up nfusion pump which administers drugs including propofol into the patient.
Doctor 2: Dr Zhu Xiu Chun @ Dr Myint Myint Kyi - monitor the patient's vital signs. Continuous oxygen supply, equipment measuring the vital signs was in place.
Said readings were within an acceptable range, no snoring or other abnormal respiratory movement to sugestg that Mr Heng' airway was disturbed. If the patient did not move much, he was quite sedated and dosage of propofol would be adjusted lower. If he moved or made sounds, after making sure that vital signs were staable, the dosage would be increased. Moderate sedation - responsive to tactile sensation.
Procedure: 12.30 pm to 3.50 pm
25 minutes after end of procedue, Dr Zhu was told there was an emergency. Mr Heng was pale and unresponsive and died.
Autopsy: >10 puncture wounds in intestines, liver
Question: Mr Heng's rep said that Mr Heng did not show any overt signs of pain because he was more than moderately sedated as multiple punctures in his internal organs from liposuction would be very painful.
MINISTRY OF HEALTH GUIDELINES FOR SAFE SEDATION
1. The changes in dosage of propofol had NOT been recorded. This was unsatisfactory.
2. The patient's vital signs were recorded every 15 minutes. Every 5 minutes would be better. Vital signs include pulse rate, blood pressure, oxygen saturation
In an earlier inquest - fact finding rather than determination of who was to blame for Mr Heng's death, two experts mentioned that the patient was over-sedated.
Liposuction Death - I did not cause death, says doctor
Patient: Mr Heng went to Reves Clinic in Orchard Rd on Dec 30, 2009 for a liposuction and fat-transfer operation.
Doctor 1: Dr Jim Wong did the surgery. Set up nfusion pump which administers drugs including propofol into the patient.
Doctor 2: Dr Zhu Xiu Chun @ Dr Myint Myint Kyi - monitor the patient's vital signs. Continuous oxygen supply, equipment measuring the vital signs was in place.
Said readings were within an acceptable range, no snoring or other abnormal respiratory movement to sugestg that Mr Heng' airway was disturbed. If the patient did not move much, he was quite sedated and dosage of propofol would be adjusted lower. If he moved or made sounds, after making sure that vital signs were staable, the dosage would be increased. Moderate sedation - responsive to tactile sensation.
Procedure: 12.30 pm to 3.50 pm
25 minutes after end of procedue, Dr Zhu was told there was an emergency. Mr Heng was pale and unresponsive and died.
Autopsy: >10 puncture wounds in intestines, liver
Question: Mr Heng's rep said that Mr Heng did not show any overt signs of pain because he was more than moderately sedated as multiple punctures in his internal organs from liposuction would be very painful.
MINISTRY OF HEALTH GUIDELINES FOR SAFE SEDATION
1. The changes in dosage of propofol had NOT been recorded. This was unsatisfactory.
2. The patient's vital signs were recorded every 15 minutes. Every 5 minutes would be better. Vital signs include pulse rate, blood pressure, oxygen saturation
In an earlier inquest - fact finding rather than determination of who was to blame for Mr Heng's death, two experts mentioned that the patient was over-sedated.
698. Pterygia and glaucoma - anaesthesia in a 12-year-old dog
In Feb 2010, I operated on the old dog with two pterygia in the right eye.


The case is described at:
http://www.asiahomes.com/singaporetpvet/rabbit/rabbit.htm
Yesterday, Oct 19, 2011, I operated on this 12-year-old again. She was a happy dog as he wagged her short tail, unlike some dogs that had to be dragged into the vet surgery.
The pterygia had re-grown and covered the whole eye. Despite anti-glaucoma eye drops given by the medically knowledgeable owner, the glaucoma could not be cured. Now the ptergygia had covered the whole cornea as well, nearly 100%.
"I thought you spoke to the human eye expert regarding opening a hole in the sclera to drain the high eye pressure?" I asked her the day before yesterday when the dog was admitted. She had made a special appointment to see me at 10 am as she wanted me to do her dog's operation to take out the eyeball.
"In human glaucoma surgery," she said, "a stent has to be inserted into the eye to drain off the excess fluid."
"The dog will not tolerate a stent inside her eye," I said. So she gave the usual anti-glaucoma eye drops and they worked apparently. Till the pterygia over-grew the cornea by 100%. Eyeball enucleation was the only alternative.
Now the surgery is relatively easy but the main issue is that the vet must produce a dog alive at the end of surgery. Death on the operating table is not an option. I was much apprehensive about doing anaesthesia on this old dog, much beloved by the family members.
I had operated on a 16-year-old with several large circum-anal tumours. Just as I completed removal of the tumours, the dog's tongue turned snow white. There was no hope as there must be a rupture of the blood vessel in the inside, probably the liver as the total whiteness of the tongue meant massive bleeding usually.
This dog had liver disease as evident by the blood test. I wanted to postpone the operation to a Thursday, having put the dog on antibiotics for at least a week. However, the owners had to take leave and so I operated on a Monday as scheduled earlier. As to whether delaying by 3 days would make a difference to survival, it is not possible to forecast. Anaesthesia in old dogs are high risk and I don't take such cases unless the owners and family members are well aware of the tremendous risks involved. No vet cannot be 100% successful in anaesthesia of old dogs. Deaths on the operating table are extremely emotional and so I prefer not to operate but some cases just can't live a good quality of life without surgery.
As part of coaching of my assistant Mr Min, I will record what had been done for the benefit of vet students. In vet school, the anaesthetic theories are sound and if you adopt them to the letter, you are supposed to be successful.
In practice, the health and age of the old dog make veterinary anaesthesia highly risky as this will be the case in human anaesthesia. This is what I did for this old dog.
Oct 18, 2011. The dog was admitted. The owner said the dog ate well and was normal.

A DAY BEFORE OPERATION.
1. Blood test was taken.
2. No X-ray was done to reduce costs but X-ray of the chest and ECG are done in the Singapore General Hospital when I was operated on.
3. I gave an IV dextrose saline 500 ml + duphalyte 50 ml to this dog. IV baytril given.
OPERATION DAY
1. Blood test was normal for this dog. This was good news.
2. Pre-op examination. The pulse quality was poor and the pulse was barely palpable. This was bad news. Other than that the temperature and respiration were normal.
3. Sedation. This is how I coached Mr Min on the dosage of Zoletil as I asked him to learn by writing on a piece of paper the dosage calculations.
The calculation is as follows:
In the dog, the maximum Zoletil 100 is 10 mg/kg. The dog weighed 24.5 kg and would need 245 mg. Therefore the volume of Zoletil 100 (100mg/ml) should be 245/100 = 2.45 ml.
However, I was using Zoletil 50. In theory, I should give 4.90 ml IV as Zoletil 50 is half the strength of Zoletil 100. Mr Min said he understood.
I took out a 1-ml syringe and gave the dog Zoletil 50 at 0.5 ml IV. This is 10% of the calculated dose. The 12-year-old dog was unable to stand 2 minutes after the injection. For a young dog, the dosage would be ineffective.
4. Isoflurane gas by mask 10 minutes later. 5% given initially.
"Check the left eyelid blinking reflex," I told Min as he was looking at the chest movements. "When the eye white (sclera) is seen, that means the dog is in surgical anaesthesia. That means the eyeball has rolled downwards. This is such a simple method of assessing the onset of surgical anaesthesia but many vet assistants don't use this method but rely on chest movements. "When chest movements stop," I said to Min, "It is already very serious heart failure. Put your finger onto the eyelids and see whether they blink."
It takes a lot of patience to repeat instructions to new people. Life is like that. Some know it faster than others. In human general hospitals you have the specialist anaesthetist to focus on anaesthesia but for vets in most practices, the sole responsibility is the vet surgeon.
5. Intubation. When the blink reflex was gone, I intubated this dog. However, she had problem taking the isoflurane gas by tube. Her chest movements were rapid and irregularly fast. I took out the tube, put on mask again. There was some froth seen in the endotracheal tube.
6. Atropine 0.5 ml IM and Lasix 1 vial 2 ml IV were given.
7. I intubated again. The dog reacted as if the tube was irritating. It gave vomiting sounds, as if one is clearing the throat. No vomitus. Yet the dog appeared to want to vomit. So I took out the tube and gave gas by mask.
The dog struggled to get up. "Give mask at 3% isoflurane, not 5%," I said to Min who was to be focused on anaesthesia. "It will take a long time at 3% but it is safer than 5%."
8. SURGERY
The dog kept curling his tongue upwards at one stage, during mask anaesthesia. Finally he was down to be operated. I cut 2 cm at the lateral canthus, cut the conjunctiva circumference of the sclera. The eyeball collapased but was taken out. I did not pull out the globe hard as this would traumatise the optic nerve and affect the eyesight of the normal left eye. The optic nerve could not be ligated. It was cut. Bleeding was profuse. Bleeding controlled by 5 swabs after cutting the eyeball and taking it out.
9. SURGERY DURATION
Nearly 1.5 hours due to the reactions of the old dog in being anaesthesized by intubation. He had some respiratory secretions and at one time, he panted or hyperventilated for over a few minutes. There are dogs that can't be anaesthesized using intubation which is the favoured ideal method of giving gas anaesthesia as they reacted to having a tube in their trachea. Why, I don't know. It happens in very rare cases. Changing to mask resolves the problem as in this case.
By mask, it was smooth and uneventful. The dog woke up immediately after the last stitch.
10. POST-OP. Tolfedine 2.5 ml IM and SC (2 parts). Baytril tablets 3 days. Then clavulox for another 10 days. Tolfedine tablets 5 days as painkillers.
11. GOES HOME IN THE EVENING. The dog was awake within 5 minutes after end of anaesthesia. E-collar. The eyeball was swollen but no bleeding. I had put in 2 layers. 2/0 absorbable PDS to stitch up the conjunctiva (cut edges after excising the eyeball circumferentially. Then I stitch up the eyelid (excised 3 mm margin leaving 0.5 mm of medial canthus eyelid uncut). Pictures shown. What the owner wanted was a dog alive and her trust that I could deliver. It was a happy ending.
CARRYING A BIG DOG
I persisted in teaching Min how to carry the big dog without bending his back. I taught Nicole the 21-year-old girl who wanted to study vet medicine the same technique. Girls must carry big dogs too if they want to be a vet and equality and respect in this veterinary world!


The case is described at:
http://www.asiahomes.com/singaporetpvet/rabbit/rabbit.htm
Yesterday, Oct 19, 2011, I operated on this 12-year-old again. She was a happy dog as he wagged her short tail, unlike some dogs that had to be dragged into the vet surgery.
The pterygia had re-grown and covered the whole eye. Despite anti-glaucoma eye drops given by the medically knowledgeable owner, the glaucoma could not be cured. Now the ptergygia had covered the whole cornea as well, nearly 100%.
"I thought you spoke to the human eye expert regarding opening a hole in the sclera to drain the high eye pressure?" I asked her the day before yesterday when the dog was admitted. She had made a special appointment to see me at 10 am as she wanted me to do her dog's operation to take out the eyeball.
"In human glaucoma surgery," she said, "a stent has to be inserted into the eye to drain off the excess fluid."
"The dog will not tolerate a stent inside her eye," I said. So she gave the usual anti-glaucoma eye drops and they worked apparently. Till the pterygia over-grew the cornea by 100%. Eyeball enucleation was the only alternative.
Now the surgery is relatively easy but the main issue is that the vet must produce a dog alive at the end of surgery. Death on the operating table is not an option. I was much apprehensive about doing anaesthesia on this old dog, much beloved by the family members.
I had operated on a 16-year-old with several large circum-anal tumours. Just as I completed removal of the tumours, the dog's tongue turned snow white. There was no hope as there must be a rupture of the blood vessel in the inside, probably the liver as the total whiteness of the tongue meant massive bleeding usually.
This dog had liver disease as evident by the blood test. I wanted to postpone the operation to a Thursday, having put the dog on antibiotics for at least a week. However, the owners had to take leave and so I operated on a Monday as scheduled earlier. As to whether delaying by 3 days would make a difference to survival, it is not possible to forecast. Anaesthesia in old dogs are high risk and I don't take such cases unless the owners and family members are well aware of the tremendous risks involved. No vet cannot be 100% successful in anaesthesia of old dogs. Deaths on the operating table are extremely emotional and so I prefer not to operate but some cases just can't live a good quality of life without surgery.
As part of coaching of my assistant Mr Min, I will record what had been done for the benefit of vet students. In vet school, the anaesthetic theories are sound and if you adopt them to the letter, you are supposed to be successful.
In practice, the health and age of the old dog make veterinary anaesthesia highly risky as this will be the case in human anaesthesia. This is what I did for this old dog.
Oct 18, 2011. The dog was admitted. The owner said the dog ate well and was normal.

A DAY BEFORE OPERATION.
1. Blood test was taken.
2. No X-ray was done to reduce costs but X-ray of the chest and ECG are done in the Singapore General Hospital when I was operated on.
3. I gave an IV dextrose saline 500 ml + duphalyte 50 ml to this dog. IV baytril given.
OPERATION DAY
1. Blood test was normal for this dog. This was good news.
2. Pre-op examination. The pulse quality was poor and the pulse was barely palpable. This was bad news. Other than that the temperature and respiration were normal.
3. Sedation. This is how I coached Mr Min on the dosage of Zoletil as I asked him to learn by writing on a piece of paper the dosage calculations.
The calculation is as follows:
In the dog, the maximum Zoletil 100 is 10 mg/kg. The dog weighed 24.5 kg and would need 245 mg. Therefore the volume of Zoletil 100 (100mg/ml) should be 245/100 = 2.45 ml.
However, I was using Zoletil 50. In theory, I should give 4.90 ml IV as Zoletil 50 is half the strength of Zoletil 100. Mr Min said he understood.
I took out a 1-ml syringe and gave the dog Zoletil 50 at 0.5 ml IV. This is 10% of the calculated dose. The 12-year-old dog was unable to stand 2 minutes after the injection. For a young dog, the dosage would be ineffective.
4. Isoflurane gas by mask 10 minutes later. 5% given initially.
"Check the left eyelid blinking reflex," I told Min as he was looking at the chest movements. "When the eye white (sclera) is seen, that means the dog is in surgical anaesthesia. That means the eyeball has rolled downwards. This is such a simple method of assessing the onset of surgical anaesthesia but many vet assistants don't use this method but rely on chest movements. "When chest movements stop," I said to Min, "It is already very serious heart failure. Put your finger onto the eyelids and see whether they blink."
It takes a lot of patience to repeat instructions to new people. Life is like that. Some know it faster than others. In human general hospitals you have the specialist anaesthetist to focus on anaesthesia but for vets in most practices, the sole responsibility is the vet surgeon.
5. Intubation. When the blink reflex was gone, I intubated this dog. However, she had problem taking the isoflurane gas by tube. Her chest movements were rapid and irregularly fast. I took out the tube, put on mask again. There was some froth seen in the endotracheal tube.
6. Atropine 0.5 ml IM and Lasix 1 vial 2 ml IV were given.
7. I intubated again. The dog reacted as if the tube was irritating. It gave vomiting sounds, as if one is clearing the throat. No vomitus. Yet the dog appeared to want to vomit. So I took out the tube and gave gas by mask.
The dog struggled to get up. "Give mask at 3% isoflurane, not 5%," I said to Min who was to be focused on anaesthesia. "It will take a long time at 3% but it is safer than 5%."
8. SURGERY
The dog kept curling his tongue upwards at one stage, during mask anaesthesia. Finally he was down to be operated. I cut 2 cm at the lateral canthus, cut the conjunctiva circumference of the sclera. The eyeball collapased but was taken out. I did not pull out the globe hard as this would traumatise the optic nerve and affect the eyesight of the normal left eye. The optic nerve could not be ligated. It was cut. Bleeding was profuse. Bleeding controlled by 5 swabs after cutting the eyeball and taking it out.
9. SURGERY DURATION
Nearly 1.5 hours due to the reactions of the old dog in being anaesthesized by intubation. He had some respiratory secretions and at one time, he panted or hyperventilated for over a few minutes. There are dogs that can't be anaesthesized using intubation which is the favoured ideal method of giving gas anaesthesia as they reacted to having a tube in their trachea. Why, I don't know. It happens in very rare cases. Changing to mask resolves the problem as in this case.
By mask, it was smooth and uneventful. The dog woke up immediately after the last stitch.
10. POST-OP. Tolfedine 2.5 ml IM and SC (2 parts). Baytril tablets 3 days. Then clavulox for another 10 days. Tolfedine tablets 5 days as painkillers.
11. GOES HOME IN THE EVENING. The dog was awake within 5 minutes after end of anaesthesia. E-collar. The eyeball was swollen but no bleeding. I had put in 2 layers. 2/0 absorbable PDS to stitch up the conjunctiva (cut edges after excising the eyeball circumferentially. Then I stitch up the eyelid (excised 3 mm margin leaving 0.5 mm of medial canthus eyelid uncut). Pictures shown. What the owner wanted was a dog alive and her trust that I could deliver. It was a happy ending.
CARRYING A BIG DOG
I persisted in teaching Min how to carry the big dog without bending his back. I taught Nicole the 21-year-old girl who wanted to study vet medicine the same technique. Girls must carry big dogs too if they want to be a vet and equality and respect in this veterinary world!
Wednesday, October 19, 2011
Follow up video production on the Chihuahua with oro-nasal fistual and lessons learnt
Oro-nasal fistula in an old Chihuahua - Part 2. The follow-up
show details Oct 16 (3 days ago)
Hi
I find your joint-production video much alive and interesting with 2 people narrating. It is just like a duet with two people singing. It is much more responsive and fun.
I need both of you to help me produce the follow up video on Daphne's case so that I can show at the AVA Responsible Pet Ownership 2011 talk.
1. Please do me a favour to produce the video together with .... The URL is at:
http://2010vets.blogspot.com/2011/10/690-follow-up-oro-nasal-fistula-old-dog.html
MAKE IT COME ALIVE as the dog is already dead and I have no video of her.
2. As regards music inside your video, it is a great idea. I love it. It makes me awake and alert. Not so boring. Great idea.
However, I wonder if there are copyrights issue. It is best to produce your own music or get permission from the young music-producing students (if there are any!).
3. Errors - FIV in a stray cat.
3.1 Antigens
In one slide, you say "Antibodies". Pl check. I believe it should be "antigens".
I love the red finger nails of the "Vet". It is so much interesting. Unfortunately Dr Vanessa does not paint her nails red or at all!
Best wishes. Let me know if you have questions.
-----------------------------------------------------------
show details Oct 18 (1 day ago)
Hi Dr Sing,
Thanks for your kind remarks! ... and I will be glad to produce the video for you, but we are not quite sure what a "follow-up" video is about though!
Looking forward to your reply,
Name
----------------------------------------------------------------------
E-MAIL REPLY FROM DR SING DATED OCT 19, 2011
1. Follow up means "what happens to the dog" since I last saw him.
The last time I saw him was the video produced by Daphne Ng. This is at:
http://www.youtube.com/user/99pups#p/u/1/5AWHpWYWgy4
2. The video ended with the operation done successfully. The dog goes home.
The follow up:
2.1 SEVEN DAYS LATER - mum happy. No need to clean up the non-healing wound as the infected tooth root had been extracted. Healing takes place.
2.2 SEVEN MONTHS LATER, Upper respiratory tract infection. Treated OK.
2.3 EIGHT MONTHS LATER, Dog died. What was the cause? Old age? No. It was actually a septicaemia due to pyometra.
Seriously ill. Anaemic. IV drip. No hope.
"Any bleeding recently?" I asked. The dog was not spayed and could have got an infected womb. This is called PYOMETRA.
"No," the son said.
"Yes, around 2 months ago....(see my notes) and case at:
http://www.sinpets.com/dogs/20100651tartar_plaque_dental_scaling_dogs_singapore_ToaPayohVets.htm
CONCLUSION
The dog would have lived to a ripe old age if the mother had her spayed or told the son that the dog had been bleeding and contact the vet. The son is a busy marketing man and so he is not the care-giver. Unfortunately, the mother had not communicated with him about the bleeding episode which was a case of PYOMETRA. The bacteria in the infected womb continued its attack on the dog, spreading toxins and infecting other organs. When the dog came to the vet, she was at death's door.
The son was actually the one who loves this dog as shown by his actions. But he did not know the dog had a serious bleeding problem as the mum did not tell him. In retrospect, spaying this dog early would have had prevented this death. But many Singapore owners feel that it is "cruel" to spay or neuter a dog.
This is the new-age thinking but such owners need to check their dogs daily to ensure that there are no such illness or growing tumours during old age and get early vet treatment.
------------------------------------------------------------------------------------------------------------------------------
I need your help to create a dialogue. C... represents the vet asking questions (a rough tone). You represent the mum. C... has to represent the young man (a different tone of voice of a man of his age). This makes the story much more interesting than one person narrating.
Pl let me know if you need more info. Bye for now.
show details Oct 16 (3 days ago)
Hi
I find your joint-production video much alive and interesting with 2 people narrating. It is just like a duet with two people singing. It is much more responsive and fun.
I need both of you to help me produce the follow up video on Daphne's case so that I can show at the AVA Responsible Pet Ownership 2011 talk.
1. Please do me a favour to produce the video together with .... The URL is at:
http://2010vets.blogspot.com/2011/10/690-follow-up-oro-nasal-fistula-old-dog.html
MAKE IT COME ALIVE as the dog is already dead and I have no video of her.
2. As regards music inside your video, it is a great idea. I love it. It makes me awake and alert. Not so boring. Great idea.
However, I wonder if there are copyrights issue. It is best to produce your own music or get permission from the young music-producing students (if there are any!).
3. Errors - FIV in a stray cat.
3.1 Antigens
In one slide, you say "Antibodies". Pl check. I believe it should be "antigens".
I love the red finger nails of the "Vet". It is so much interesting. Unfortunately Dr Vanessa does not paint her nails red or at all!
Best wishes. Let me know if you have questions.
-----------------------------------------------------------
show details Oct 18 (1 day ago)
Hi Dr Sing,
Thanks for your kind remarks! ... and I will be glad to produce the video for you, but we are not quite sure what a "follow-up" video is about though!
Looking forward to your reply,
Name
----------------------------------------------------------------------
E-MAIL REPLY FROM DR SING DATED OCT 19, 2011
1. Follow up means "what happens to the dog" since I last saw him.
The last time I saw him was the video produced by Daphne Ng. This is at:
http://www.youtube.com/user/99pups#p/u/1/5AWHpWYWgy4
2. The video ended with the operation done successfully. The dog goes home.
The follow up:
2.1 SEVEN DAYS LATER - mum happy. No need to clean up the non-healing wound as the infected tooth root had been extracted. Healing takes place.
2.2 SEVEN MONTHS LATER, Upper respiratory tract infection. Treated OK.
2.3 EIGHT MONTHS LATER, Dog died. What was the cause? Old age? No. It was actually a septicaemia due to pyometra.
Seriously ill. Anaemic. IV drip. No hope.
"Any bleeding recently?" I asked. The dog was not spayed and could have got an infected womb. This is called PYOMETRA.
"No," the son said.
"Yes, around 2 months ago....(see my notes) and case at:
http://www.sinpets.com/dogs/20100651tartar_plaque_dental_scaling_dogs_singapore_ToaPayohVets.htm
CONCLUSION
The dog would have lived to a ripe old age if the mother had her spayed or told the son that the dog had been bleeding and contact the vet. The son is a busy marketing man and so he is not the care-giver. Unfortunately, the mother had not communicated with him about the bleeding episode which was a case of PYOMETRA. The bacteria in the infected womb continued its attack on the dog, spreading toxins and infecting other organs. When the dog came to the vet, she was at death's door.
The son was actually the one who loves this dog as shown by his actions. But he did not know the dog had a serious bleeding problem as the mum did not tell him. In retrospect, spaying this dog early would have had prevented this death. But many Singapore owners feel that it is "cruel" to spay or neuter a dog.
This is the new-age thinking but such owners need to check their dogs daily to ensure that there are no such illness or growing tumours during old age and get early vet treatment.
------------------------------------------------------------------------------------------------------------------------------
I need your help to create a dialogue. C... represents the vet asking questions (a rough tone). You represent the mum. C... has to represent the young man (a different tone of voice of a man of his age). This makes the story much more interesting than one person narrating.
Pl let me know if you need more info. Bye for now.
696. Email query about toilet training
I am Dr Sing from Toa Payoh Vets. Thank you for your email.
Basically, you need to confine him for the first 2-4 weeks and let out only after he has pooped. If not, you can't be successful. An example of my advice to a puppy owner is at:
http://www.sinpets.com/F5/20111023puppy-toilet-training-paper-or-grate-not-both-singapore-toapayohvets.htm
Best wishes.
On Tue, Oct 18, 2011 at 4:53 PM, ...@hotmail.com> wrote:
Hi,
I adopted a 2yrs plus Maltese in Jun this yr,been trying to toilet train him for the past 3months.I've tried scolding him,beating him,dripping house-breaking aid on the newspaper but nothin seem to work.It's real frustrating when I see his poos & pees in the whole house after I got Home from work.Feel like caging him up when I go to work but feel bad about caging him up.I moped the floor with dettol but he will still pee at the same spot again.Can you kindly teach me how to toilet train him properly?Thks.
Name
Sent from my iPhone
E-MAIL REPLY FROM DR SING DATED OCT 19, 2011
I am Dr Sing from Toa Payoh Vets. Thank you for your email.
Basically, you need to confine him for the first 2-4 weeks and let out only after he has pooped. If not, you can't be successful. An example of my advice to a puppy owner is at:
http://www.sinpets.com/F5/20111023puppy-toilet-training-paper-or-grate-not-both-singapore-toapayohvets.htm
Best wishes.
Basically, you need to confine him for the first 2-4 weeks and let out only after he has pooped. If not, you can't be successful. An example of my advice to a puppy owner is at:
http://www.sinpets.com/F5/20111023puppy-toilet-training-paper-or-grate-not-both-singapore-toapayohvets.htm
Best wishes.
On Tue, Oct 18, 2011 at 4:53 PM, ...@hotmail.com> wrote:
Hi,
I adopted a 2yrs plus Maltese in Jun this yr,been trying to toilet train him for the past 3months.I've tried scolding him,beating him,dripping house-breaking aid on the newspaper but nothin seem to work.It's real frustrating when I see his poos & pees in the whole house after I got Home from work.Feel like caging him up when I go to work but feel bad about caging him up.I moped the floor with dettol but he will still pee at the same spot again.Can you kindly teach me how to toilet train him properly?Thks.
Name
Sent from my iPhone
E-MAIL REPLY FROM DR SING DATED OCT 19, 2011
I am Dr Sing from Toa Payoh Vets. Thank you for your email.
Basically, you need to confine him for the first 2-4 weeks and let out only after he has pooped. If not, you can't be successful. An example of my advice to a puppy owner is at:
http://www.sinpets.com/F5/20111023puppy-toilet-training-paper-or-grate-not-both-singapore-toapayohvets.htm
Best wishes.
Tuesday, October 18, 2011
695. Unacceptable veterinary advices

Sometimes it may be wise to pass up a case rather than to offer unacceptable veterinary advices as they do stress out the hamster owner and force her family members or mother to seek another opinion.
If you add value to the hamster owner by offering alternative advices other than unacceptable advices, you may retain the goodwill and that is good for you.
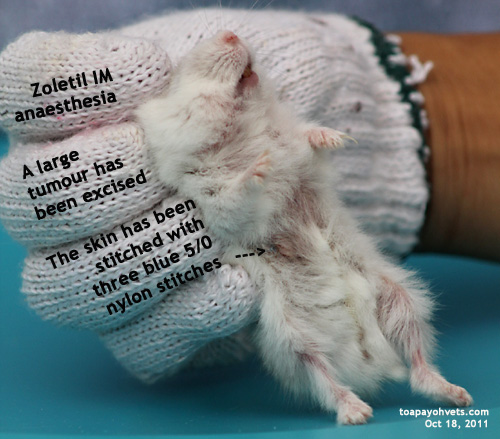

Case report at:
Toa Payoh Vets webpage
http://www.sinpets.com/F6/20111009unacceptable-veterinary-advices-hamster-tumouors-singapore_ToaPayohVets.htm
694. Two educational videos produced by two Temasek Poly Vet Tech students
We had fun producing these two video to educate pet owners and vet students. I hope you like it. The vet with the red nails is not Dr Vanessa. I seldom see lady vets in small animal practice with painted nails but times have had changed and I may be incorrect!

FIV in a stray cat
http://www.youtube.com/watch?v=ntHweZD49ec

Cystitis in a male dog
http://www.youtube.com/watch?v=HvV-00dDRg4

FIV in a stray cat
http://www.youtube.com/watch?v=ntHweZD49ec
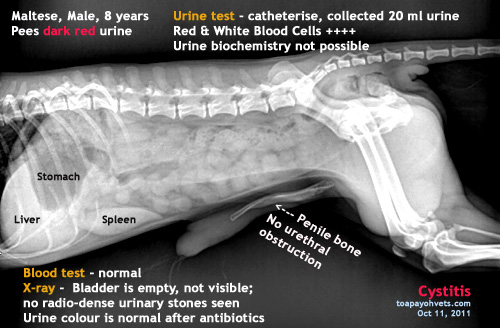
Cystitis in a male dog
http://www.youtube.com/watch?v=HvV-00dDRg4
693. Anaesthesizing a roborovski hamster
Laughter is not the best medicine in the Roborovski hamster anaesthesia
Dr Sing Kong Yuen, BVMS (Glasgow), MRCVS
18 October, 2011
toapayohvets.com
Be Kind To Pets
Veterinary Education
Project 2010-0129
The young woman said to me when I answered the phone: "I have decided to have the lump taken out by Dr Julia. Last week, he had been given antibiotics but the lump is still present."
"When can you bring the Roborovski hamster to the Surgery?" I asked.
"After work. It will be after 8 pm."
I was still working at this time and so I decided to operate together with Dr Julia and my assistant Min.
The instruments were prepared. "Put the hamster into the container and count 1 to 5," I said to Min as he inserted the endotracheal tube into the container. Min is not used to count loudly as this counting aloud is not part of his culture. "Start counting," I have had told Min that he has to do as instructed as this is part of the procedure for anaesthesia of dwarf hamsters. Otherwise, he may as well be his own boss.
"Accept instructions from your boss when you are an employee rather than do your own thing. When you become the boss of your practice, you expect your employees to follow your instructions. Otherwise, how can you trust your employee when you are not around? "
It takes time and patience to change the mindset of the average younger employee as they have their own ideas of doing things "better". This is the culture of the young ones and I accept this is the new world.
Now Min said aloud solemnly in his gruffly voice: "One... two...three..."
Dr Julia burst out laughing and so he stopped.
I said: "5 seconds of the 5% isoflurane anaesthesia is enough. Take the hamster out of the container to operate. If the hamster moves, repeat for another 5 seconds. The Roborovski is a very small hamster compared to the average dwarf hamster and so you have to be very careful. It is very hard to see whether he is sleepy or not as he is an active speedy fellow."
There was no problem. Dr Teo extracted one big fatty tumour. I said: "Stitch up with the 6/0 absorbable suture now!" It was a big tumour of 0.5mm x 0.5mm x 0.3mm. The surgery must be quickly completed as repeated gas anaesthesia will kill this hamster.
But it was not complete. Min said in his muffled voice: "There is one more lump,"
I was surprised as the fatty tumour had a twin. This was taken out and the skin quickly stitched with four interrupted sutures. The hamster woke up and walked like a drunk. I quickly had him put into the cage, just in case he rocketed off the operating table and fell on the floor. Roborovski hamsters don't walk. They sprint. This was a two-year old, much beloved by the young couple. Still, the vet must be alert as old does not mean less speedy as in an old man compared to a young one.
Anaesthesia in Roborovski hamsters needs to be very careful. The easy part is the surgery if the tumour can be shelled out as in this case. The couple came back at 9 pm and took the hamster home. This was a happy ending. Laughter is the best medicine but in hamster anaesthesia, I discourage any jokes or chatter as there is a great need to focus on anaesthesia.





4638 - 4643. Anaesthesia of the Roborovski hamster at Toa Payoh Vets
Every hamster that survives the surgery builds up the reputation of
Toa Payoh Vets as the place to go for hamster surgeries. Unlike the Singapore hospitals where you have a specialist anaesthetist and a specialist surgeon, the vet is both and many deaths on the operating table are due to a lack of focus by the assistant. So idle chatter and jokes are out if the vet and his assistant is doing anaesthesia and surgery and serious about getting excellent surgical outcomes.
No point having a perfect surgery done when the patient has had died on the operating table. The only outcome the hamster or any pet owner wants is a pet alive and going home, not a dead one. So I have been very careful about anaesthesia in my 30 years of practice.

Webpage at:
http://www.sinpets.com/F6/20111029roborovski-hamster-anaesthetic-success-singapore-toapayohvets.htm
Dr Sing Kong Yuen, BVMS (Glasgow), MRCVS
18 October, 2011
toapayohvets.com
Be Kind To Pets
Veterinary Education
Project 2010-0129
The young woman said to me when I answered the phone: "I have decided to have the lump taken out by Dr Julia. Last week, he had been given antibiotics but the lump is still present."
"When can you bring the Roborovski hamster to the Surgery?" I asked.
"After work. It will be after 8 pm."
I was still working at this time and so I decided to operate together with Dr Julia and my assistant Min.
The instruments were prepared. "Put the hamster into the container and count 1 to 5," I said to Min as he inserted the endotracheal tube into the container. Min is not used to count loudly as this counting aloud is not part of his culture. "Start counting," I have had told Min that he has to do as instructed as this is part of the procedure for anaesthesia of dwarf hamsters. Otherwise, he may as well be his own boss.
"Accept instructions from your boss when you are an employee rather than do your own thing. When you become the boss of your practice, you expect your employees to follow your instructions. Otherwise, how can you trust your employee when you are not around? "
It takes time and patience to change the mindset of the average younger employee as they have their own ideas of doing things "better". This is the culture of the young ones and I accept this is the new world.
Now Min said aloud solemnly in his gruffly voice: "One... two...three..."
Dr Julia burst out laughing and so he stopped.
I said: "5 seconds of the 5% isoflurane anaesthesia is enough. Take the hamster out of the container to operate. If the hamster moves, repeat for another 5 seconds. The Roborovski is a very small hamster compared to the average dwarf hamster and so you have to be very careful. It is very hard to see whether he is sleepy or not as he is an active speedy fellow."
There was no problem. Dr Teo extracted one big fatty tumour. I said: "Stitch up with the 6/0 absorbable suture now!" It was a big tumour of 0.5mm x 0.5mm x 0.3mm. The surgery must be quickly completed as repeated gas anaesthesia will kill this hamster.
But it was not complete. Min said in his muffled voice: "There is one more lump,"
I was surprised as the fatty tumour had a twin. This was taken out and the skin quickly stitched with four interrupted sutures. The hamster woke up and walked like a drunk. I quickly had him put into the cage, just in case he rocketed off the operating table and fell on the floor. Roborovski hamsters don't walk. They sprint. This was a two-year old, much beloved by the young couple. Still, the vet must be alert as old does not mean less speedy as in an old man compared to a young one.
Anaesthesia in Roborovski hamsters needs to be very careful. The easy part is the surgery if the tumour can be shelled out as in this case. The couple came back at 9 pm and took the hamster home. This was a happy ending. Laughter is the best medicine but in hamster anaesthesia, I discourage any jokes or chatter as there is a great need to focus on anaesthesia.





4638 - 4643. Anaesthesia of the Roborovski hamster at Toa Payoh Vets
Every hamster that survives the surgery builds up the reputation of
Toa Payoh Vets as the place to go for hamster surgeries. Unlike the Singapore hospitals where you have a specialist anaesthetist and a specialist surgeon, the vet is both and many deaths on the operating table are due to a lack of focus by the assistant. So idle chatter and jokes are out if the vet and his assistant is doing anaesthesia and surgery and serious about getting excellent surgical outcomes.
No point having a perfect surgery done when the patient has had died on the operating table. The only outcome the hamster or any pet owner wants is a pet alive and going home, not a dead one. So I have been very careful about anaesthesia in my 30 years of practice.

Webpage at:
http://www.sinpets.com/F6/20111029roborovski-hamster-anaesthetic-success-singapore-toapayohvets.htm
Monday, October 17, 2011
692. Sunday Oct 16, 2011's interesting cases
Last Sunday, Oct 9, 2011, I took the day off. Yesterday, I was present.
Case 1.
A young man came with a newly purchased English Cocker Spaniel that had passed blood in the loose stools since yesterday. The puppy had loose stools since purchase 9 days ago from a pet shop in Pasir Ris. No stools sample was available. I palpated the puppy's stomach. There was some discomfort. Other signs were normal.
This was a case study for Kim who wanted to study vet medicine and I asked her to write up the process and procedures in the diagnosis and treatment of this case. "Some vets will just give a jab for gastroenteritis and send the puppy home with medicine," I said to Kim. "However, a newly purchased puppy from a breeder or pet shop needs more thorough investigation as parvoviral infection of the gut is the first of the differential diagnosis. Parvoviruses are very common in breeding farms and pet shops.
"The puppy looks all right today but if the vet fails to check for parvovirus, he or she is actually professionally incompetent if the puppy dies a few days later of bloody diarrhoea and vomiting."
Parvovirus check -ve. Blood test taken for haematology. The puppy was warded. Will report further.
Case 2
"I don't want my 5-year-old Miniature Schnauzer to be under anaesthesia for dental scaling," the mother of a young adult daughter repeated her concern when I told her that her dog would need dental scaling. I had written on the case sheet since she came for vaccination booster last year.
"It is a vet's duty to advise," I said. "It is the owner's choice not to do it. If the vet does not advise dental check up during vaccination and the dog develops oral tumours or bad teeth or ulcers later, the owner will say that the vet has not advised me, just give vaccination only."
"In any case," the mother said, "the groomer had charged me and did the dental scaling."
"I don't see how the groomer can do it," I said as the Schnauzer moved his head here and there to prevent me and the owner from opening his mouth. "I have heard of groomers grabbing the dog and pinning it down to do dental scaling. There is one pet shop providing this service for around $120. I hear that the grooming assistant who left this pet shop was very unhappy about forcing the dog down to do the dental scaling."
"I will do it next time," the mother must be thinking I am desperate and soliciting for business.
"How much did your groomer charge?" I asked as this groomer was from a well-known chain of pet shops that has branches all over Singapore.
"$70.00" the mother said.
"$70.00 for dental work or for grooming + dental work?" I asked.
"Grooming included. I can see that the front teeth are whiter now."
"In this case, the dental work is $20 as grooming of the Schnauzer will be $50.00. It certainly is much cheaper than a vet's job."
"And no anaesthesia death. Or the dog becoming groogy after anaesthesia and can't walk properly as that is what the groomer told me!" the mother said.
"Anaesthesia is very safe in most dogs nowadays. But the vet must know what to do to ensure safe anaesthesia," I said.
It so happened that there was a Shih Tzu with his tongue protruding. That Shih Tzu had domitor 0.1 ml IV and isoflurane gas given for stitching up of the cut in the interdigit of one front paw. This was done by Vet 1 and the dog was now outside as the owner dialed for a taxi.
So the mother saw a "groogy" dog as she asked the owner what happened.
I said to my assistant, "Get me the Antisedan and bring the Shih Tzu back to the Surgery Room. I got 0.2 ml of Antisedan, added 0.2 ml of normal saline and asked Vet 1 to give it to the dog IV. The dog was alert and awake.
"As you can see," I told the mother. "There is the antidote a vet may use to wake up the dog after anaesthesia. It is up to the vet's judgment as to whether he or she wants to use it. As for me, I usually do it but not all the time as that depends on each case."
I got the Schnauzer's mother opened up finally. Thick tartar in all back teeth and some gum inflammation. The mother saw it. This is just an education for the dog owner, not a desperate hard sell to get her business. Each owner has to decide as to anaesthetic risks of dental scaling. The groomer now goes into dental scaling to take advantage of such fears and well, this is the real world.
As for the Shih Tzu, the owner wanted the interdigital wound stitched up. But Vet 1 decided to give injection, medication and wash. I intervened and told Vet 1: "The interdigital wound is not easy to heal when opened up. The dog will lick it and if a granuloma forms, the owner will be most happy. He will curse and go to another vet who will stitch up the wound belatedly. You did not advise the owner that surgery is an option. Actually the owner wanted surgery."
This Shih Tzu case showed that every vet or doctor has his or her own ideas in handling a case and no two vets will do the same thing. "Some vets advise surgery, some advise no surgery and some have no advices," I said to the Shih Tzu and Schnauzer owner. "This is the judgment of each vet."
Well, the Shih Tzu owner, being well read, wanted surgery. The Schnauzer owner agreed with him. So, you can see that a vet in private practice must give all the treatment options. Not just his or her own recommendation of conservative treatment which will be much less costly. But will it be effective in a interdigital wound recovering early and not degenerate into a interdigital granuloma or worse?
Case 1.
A young man came with a newly purchased English Cocker Spaniel that had passed blood in the loose stools since yesterday. The puppy had loose stools since purchase 9 days ago from a pet shop in Pasir Ris. No stools sample was available. I palpated the puppy's stomach. There was some discomfort. Other signs were normal.
This was a case study for Kim who wanted to study vet medicine and I asked her to write up the process and procedures in the diagnosis and treatment of this case. "Some vets will just give a jab for gastroenteritis and send the puppy home with medicine," I said to Kim. "However, a newly purchased puppy from a breeder or pet shop needs more thorough investigation as parvoviral infection of the gut is the first of the differential diagnosis. Parvoviruses are very common in breeding farms and pet shops.
"The puppy looks all right today but if the vet fails to check for parvovirus, he or she is actually professionally incompetent if the puppy dies a few days later of bloody diarrhoea and vomiting."
Parvovirus check -ve. Blood test taken for haematology. The puppy was warded. Will report further.
Case 2
"I don't want my 5-year-old Miniature Schnauzer to be under anaesthesia for dental scaling," the mother of a young adult daughter repeated her concern when I told her that her dog would need dental scaling. I had written on the case sheet since she came for vaccination booster last year.
"It is a vet's duty to advise," I said. "It is the owner's choice not to do it. If the vet does not advise dental check up during vaccination and the dog develops oral tumours or bad teeth or ulcers later, the owner will say that the vet has not advised me, just give vaccination only."
"In any case," the mother said, "the groomer had charged me and did the dental scaling."
"I don't see how the groomer can do it," I said as the Schnauzer moved his head here and there to prevent me and the owner from opening his mouth. "I have heard of groomers grabbing the dog and pinning it down to do dental scaling. There is one pet shop providing this service for around $120. I hear that the grooming assistant who left this pet shop was very unhappy about forcing the dog down to do the dental scaling."
"I will do it next time," the mother must be thinking I am desperate and soliciting for business.
"How much did your groomer charge?" I asked as this groomer was from a well-known chain of pet shops that has branches all over Singapore.
"$70.00" the mother said.
"$70.00 for dental work or for grooming + dental work?" I asked.
"Grooming included. I can see that the front teeth are whiter now."
"In this case, the dental work is $20 as grooming of the Schnauzer will be $50.00. It certainly is much cheaper than a vet's job."
"And no anaesthesia death. Or the dog becoming groogy after anaesthesia and can't walk properly as that is what the groomer told me!" the mother said.
"Anaesthesia is very safe in most dogs nowadays. But the vet must know what to do to ensure safe anaesthesia," I said.
It so happened that there was a Shih Tzu with his tongue protruding. That Shih Tzu had domitor 0.1 ml IV and isoflurane gas given for stitching up of the cut in the interdigit of one front paw. This was done by Vet 1 and the dog was now outside as the owner dialed for a taxi.
So the mother saw a "groogy" dog as she asked the owner what happened.
I said to my assistant, "Get me the Antisedan and bring the Shih Tzu back to the Surgery Room. I got 0.2 ml of Antisedan, added 0.2 ml of normal saline and asked Vet 1 to give it to the dog IV. The dog was alert and awake.
"As you can see," I told the mother. "There is the antidote a vet may use to wake up the dog after anaesthesia. It is up to the vet's judgment as to whether he or she wants to use it. As for me, I usually do it but not all the time as that depends on each case."
I got the Schnauzer's mother opened up finally. Thick tartar in all back teeth and some gum inflammation. The mother saw it. This is just an education for the dog owner, not a desperate hard sell to get her business. Each owner has to decide as to anaesthetic risks of dental scaling. The groomer now goes into dental scaling to take advantage of such fears and well, this is the real world.
As for the Shih Tzu, the owner wanted the interdigital wound stitched up. But Vet 1 decided to give injection, medication and wash. I intervened and told Vet 1: "The interdigital wound is not easy to heal when opened up. The dog will lick it and if a granuloma forms, the owner will be most happy. He will curse and go to another vet who will stitch up the wound belatedly. You did not advise the owner that surgery is an option. Actually the owner wanted surgery."
This Shih Tzu case showed that every vet or doctor has his or her own ideas in handling a case and no two vets will do the same thing. "Some vets advise surgery, some advise no surgery and some have no advices," I said to the Shih Tzu and Schnauzer owner. "This is the judgment of each vet."
Well, the Shih Tzu owner, being well read, wanted surgery. The Schnauzer owner agreed with him. So, you can see that a vet in private practice must give all the treatment options. Not just his or her own recommendation of conservative treatment which will be much less costly. But will it be effective in a interdigital wound recovering early and not degenerate into a interdigital granuloma or worse?
691. Switching from a government vet to a small animal vet
On Thu, Oct 6, 2011 ...@yahoo.com> wrote:
Dear Dr Sing,
I chanced upon your blog when I was looking up some vet related blogs. I read that you completed your bond with the PPD, then started up toapayoh vet clinic. Was it difficult to transition from a government vet to a small animal vet? How do you keep the knowledge learnt for small animals fresh in your mind as being a PPD government vet requires a completely different set of skills? Would be great if you could provide me with some advice on this issue. I've been pondering on career pathways recently and I need guidance.
Regards,
Name
E-MAIL REPLY FROM DR SING
Thank you for your email. In reply to your questions:
1. It is not difficult to change to small animal practice from regulatory practice for me as I had a mentor (an experienced senior vet) whom I spent time in the evenings (closing my practice) learning from him, assisting him, working as locum and doing house-calls.
2. Lots of reading on small animal vet journals. In 1982, when I started Toa Payoh Vets, there was no such thing as the world wide web. So, lots of reading vet articles and journals and subscription to the British and American vet journals. The PPD had a small vet library at 40 Kampong Java Road, now the K.K. Hospital.
3. For your situation, be an employee in one of the 46 vet practices in Singapore for at least two years. Choose a busy one, otherwise you would have not sufficient variety of cases. Work the night shifts and really attend to each emergency as if it was your own pet instead of being a "lazy" vet, letting the vet technicians do the hands-on blood collection, urine collection and X-rays.
Give practically free services to the dog breeders and animal activists. So much small animal veterinary work to do nowadays. Read up and discuss with mentors. Review cases done and see if there are better and more efficient and cost-effective ways to handling the case.
Add value to your employer. For example, I note that some young employee vets use more than necessary (increasing expenses to the practice and reducing the bottom-line) the sutures and materials used in surgery and treatment. This may not endear yourself to the Principal of the practice as it shows you don't care about the bottom-line. In private practice, the costs are high and you need to be aware of the economics of practice, other than the salary and benefits you are getting.
In conclusion, venturing to a new field requires a new mindset to work the long hours to achieve competence and success. Small animal private practice hours are longer and will not be similar to the regular hours of civil service as most clients are free during weekends and public holidays when the civil service vet is having time off.
Passion is required if you wish to excel. Competition is great nowadays as I expect more than 50 small animal practices to be set up in the next 5 years if you intend to open your own practice. Know the economics of practice. Add value to your employer or principal. Continuing education. Network. Be proactive in vet matters.
Phone me if you need more advice as writing advices are not as good as one-to-one talk.
E-MAIL REPLY TO DR SING DATED OCT 17, 2011
Dear Dr Sing,
Thanks so much for your reply. It has motivated me to work alot harder, and that nothing is impossible. Your advice has given me the direction I was missing before as I did not know who else to ask. Thank you once again.
Regards,
Name
Dear Dr Sing,
I chanced upon your blog when I was looking up some vet related blogs. I read that you completed your bond with the PPD, then started up toapayoh vet clinic. Was it difficult to transition from a government vet to a small animal vet? How do you keep the knowledge learnt for small animals fresh in your mind as being a PPD government vet requires a completely different set of skills? Would be great if you could provide me with some advice on this issue. I've been pondering on career pathways recently and I need guidance.
Regards,
Name
E-MAIL REPLY FROM DR SING
Thank you for your email. In reply to your questions:
1. It is not difficult to change to small animal practice from regulatory practice for me as I had a mentor (an experienced senior vet) whom I spent time in the evenings (closing my practice) learning from him, assisting him, working as locum and doing house-calls.
2. Lots of reading on small animal vet journals. In 1982, when I started Toa Payoh Vets, there was no such thing as the world wide web. So, lots of reading vet articles and journals and subscription to the British and American vet journals. The PPD had a small vet library at 40 Kampong Java Road, now the K.K. Hospital.
3. For your situation, be an employee in one of the 46 vet practices in Singapore for at least two years. Choose a busy one, otherwise you would have not sufficient variety of cases. Work the night shifts and really attend to each emergency as if it was your own pet instead of being a "lazy" vet, letting the vet technicians do the hands-on blood collection, urine collection and X-rays.
Give practically free services to the dog breeders and animal activists. So much small animal veterinary work to do nowadays. Read up and discuss with mentors. Review cases done and see if there are better and more efficient and cost-effective ways to handling the case.
Add value to your employer. For example, I note that some young employee vets use more than necessary (increasing expenses to the practice and reducing the bottom-line) the sutures and materials used in surgery and treatment. This may not endear yourself to the Principal of the practice as it shows you don't care about the bottom-line. In private practice, the costs are high and you need to be aware of the economics of practice, other than the salary and benefits you are getting.
In conclusion, venturing to a new field requires a new mindset to work the long hours to achieve competence and success. Small animal private practice hours are longer and will not be similar to the regular hours of civil service as most clients are free during weekends and public holidays when the civil service vet is having time off.
Passion is required if you wish to excel. Competition is great nowadays as I expect more than 50 small animal practices to be set up in the next 5 years if you intend to open your own practice. Know the economics of practice. Add value to your employer or principal. Continuing education. Network. Be proactive in vet matters.
Phone me if you need more advice as writing advices are not as good as one-to-one talk.
E-MAIL REPLY TO DR SING DATED OCT 17, 2011
Dear Dr Sing,
Thanks so much for your reply. It has motivated me to work alot harder, and that nothing is impossible. Your advice has given me the direction I was missing before as I did not know who else to ask. Thank you once again.
Regards,
Name
Saturday, October 15, 2011
689. AVA Responsible Pet Road Show 2011 - Two talks by Dr Sing, Toa Payoh Vets
Today: Oct 15, 2011. Need to prepare for the following talks. A video presentation will be more fun and interesting to the audience.
Examples of videos will be:
1. Cystitis in A Male Dog
2. FIV in a Stray Cat
3. Carnaissal Tooth Abscess in an old dog
4. Closed pyometra and toxaemia in a dog
5. A gigantic perineal hernia in a silkie terrier
6. Heart disease in a Golden Retriever
5. Hamster tumours
6. Hamster warts
AVA RESPONSIBLE PET OWNERSHIP ROAD SHOW
CHANGI EXPO Nov 12 and 13, 2011
I will be giving two talks as follows:
Sat Nov 12, 2011 1.30 - 2pm Some common diseases in Singapore dogs - cases seen at Toa Payoh Vets
Sun Nov 13, 2011 3.30 - 4pm Tumoours and warts in Singapore hamsters - cases seen at Toa Payoh Vets
Examples of videos will be:
1. Cystitis in A Male Dog
2. FIV in a Stray Cat
3. Carnaissal Tooth Abscess in an old dog
4. Closed pyometra and toxaemia in a dog
5. A gigantic perineal hernia in a silkie terrier
6. Heart disease in a Golden Retriever
5. Hamster tumours
6. Hamster warts
AVA RESPONSIBLE PET OWNERSHIP ROAD SHOW
CHANGI EXPO Nov 12 and 13, 2011
I will be giving two talks as follows:
Sat Nov 12, 2011 1.30 - 2pm Some common diseases in Singapore dogs - cases seen at Toa Payoh Vets
Sun Nov 13, 2011 3.30 - 4pm Tumoours and warts in Singapore hamsters - cases seen at Toa Payoh Vets
688. Two educational vet videos produced by two students - Cystitis in a dog, FIV in a stray cat
GREAT WORK DONE BY TWO TEMASEK POLYTECHNIC VET TECHNOLOGY STUDENTS
in OCT 14, 2011.
Thank you for your help in producing the two videos.
You had the excellent idea for two parties to narrate the video as it makes the video much more interesting to watch.
Can hear clearly an loudly.
May need to do some editing as "diagnosis" is spelt as "diagnosi" etc.
It was great to get to know both of you.
Best wishes to your studies. Thank you again.
The URL are:
http://www.youtube.com/watch?v=HvV-00dDRg4&NR=1
CYSTITIS IN A MALE DOG
http://www.youtube.com/watch?v=ntHweZD49ec&feature=related
FIV IN A STRAY CAT
P.S. The two students did not want to be acknowledged. So, they gave me all the credit.
in OCT 14, 2011.
Thank you for your help in producing the two videos.
You had the excellent idea for two parties to narrate the video as it makes the video much more interesting to watch.
Can hear clearly an loudly.
May need to do some editing as "diagnosis" is spelt as "diagnosi" etc.
It was great to get to know both of you.
Best wishes to your studies. Thank you again.
The URL are:
http://www.youtube.com/watch?v=HvV-00dDRg4&NR=1
CYSTITIS IN A MALE DOG
http://www.youtube.com/watch?v=ntHweZD49ec&feature=related
FIV IN A STRAY CAT
P.S. The two students did not want to be acknowledged. So, they gave me all the credit.
687. Abusing veterinary staff
On Thursday Oct 15, 2011, I paid a visit to my mentor, a senior vet. I asked if he has an X-ray of urinary stones in the cat as I had not seen one in over 30 years of practice. He said that cats usually suffer from urinary sand and he had none. At that time, he showed me an X-ray of the Chihuahua with at least 10 urinary stones stuck in the os penis. The bladder was full due to urethral obstruction and there were no radio-dense stones seen in the bladder. A younger vet had referred this dog to him. Well, this is the type of surgery with wounds that are difficult to heal sometimes and so it is wise to refer to this senior vet.
"Do you use urohydropropulsion by syringing saline to flush back the stones to the bladder and then remove them from the bladder?" I asked him, just in case I can get some tips from his long hours spent in veterinary medicine and surgery. He is likely the most experienced vet in Singapore as he puts in the long hours over 40 years of practice when many vets would have been burnt out or work short hours.
Obviously the most efficient and simple way is to cut a hole into the urethra behind the penile bone and take the stones out. Then stitch up the urethra. Where the complications come in is that the urethra does not close properly and the male Chihuahua will leak urine through this hole, soiling the apartment floor. If the healing is good, the male dog pees normally.
"No point opening up the bladder as there are not stones seen inside," he said. "The bladder is full and any stones inside may not be visible but are likely to be small."
On another matter, I was surprised when he asked me whether the presence of 50 veterinary practices nowadays can be supported by the number of dogs and cats.
He said: "30 years ago, there were only 5 practices - myself, Deveraj, Cho Chak Nam, Animal Clinic and The Veterinary Surgery. I estimated that the number of dogs have increased twice but the number of vet practice has increased 10X. Many dog owners did not license their dogs in the old days. What do you think (of the impact of so many vet practices)?"
"I estimated that the number of dogs would have increased at least 3X based on the number of licences issued and the fact that micro-chipping of dogs is compulsory and enforcement action for unlicensed dogs," I replied. "Some newer vet practices will not be profitable as prices will have to be below costs for such practices in order to attract clientele.
"However, Singaporeans tend to go for proximity and therefore, convenience and affordable costs will bring some business to the new practices and with good personality, some of the newer practices will do very well. Experience and white hairs don't count for most Singaporeans. It is proximity and personality of the younger vets."
I was surprised to see a notice on his reception counter educating members of the public not to be abusive towards his staff. Such notices have been put up by the Singapore General Hospital some 2 years ago but no longer seen and are put up in some government offices or statutory boards like the National Library Board.
Life must be more stressful for some members of the public nowadays such that they become abusive at serving staff. Three Sundays ago, I was on the receiving end of the abusive dog owner who made an appointment to consult Dr Vanessa. He was rude and shouting inside the consultation room where Dr Vanessa and I were present while Dr Vanessa examined his dog's paw. Dr Vanessa kept mum and I left the room, forgetting about the behaviour. At the end of consultation, this man forced his way into the Surgery room where I was consulting with another dog owner and shouted at me to go to the back of the practice and pay him for advice as to what's wrong with my management of Toa Payoh Vets. He was loud and his adult son pulled him away. Such type of clients should be banned and I told Dr Vanessa how to handle such clients in the future. If she keeps silent, she encourages repetition of anger and abuse to me and the staff, except to herself.
Another of Dr Vanessa's client, a young Indian man, punched his fist into the gypsum wall of the consultation room when his family members and him were performing rites on his old dog with oral tumours. The dog had just been put to sleep by Dr Vanessa and the family had prepared some flowers and funeral paraphernalia for the farewell ritual and to wait for the cremation man. Dr Vanessa left the room to attend to another dog at the kennels. I was at the reception area. Suddenly, there was a loud explosive bang on the wall separating the reception from the consultation room. I went inside the consultation room to investigate the bang and since the family was grieving, I did not raise any complaint about the damage.
You can see the dent on the wall when you enter the consultation room of Toa Payoh Vets.
I spoke to Dr Vanessa recently about these two clients of hers. In my 30 years of veterinary practice, I had not encountered such rage. I told her that she had to let such clients know that their behaviour is not acceptable by me, the Principal. If she keeps silent, such behaviour will continue.
"What will you do?" she asked me. "I don't talk to them about their behaviour but focus on consultation."
Well, such anger was not directed at her in the first place. In fact, she was the doctor in charge and consulted. But ignoring such misbehaviour is not good for the team as she obviously cannot work alone. If the vet does not care for the team, the vet should not be accredited to work at Toa Payoh Vets. This is my policy.
This is how she should handle this matter.
I said: "Ask your client courteously - 'Is there some deficiency in my veterinary services to you? How may I help you to improve our veterinary services?"
This is better than keeping silent. I am prepared to ban such abusive clients from Toa Payoh Vets even if they say Dr Vanessa is the best vet in Singapore! Poor anger management is very dangerous to veterinary staff as some angry males do assault and kill. So, it is wise that the Principal or the associate vet know how to handle such clients. Putting up "educational notices" on the walls of Toa Payoh Vets telling clients not to abuse staff is not the answer, in my opinion. This is because the vast majority of Toa Payoh Vets clientele is excellent. The abusive ones make up 1% of the clientele and so I don't permit such "educational notices" to be put up.
The younger generation is into a new golden age of the internet. Those that can manage their anger will prosper. As for those that cannot, the service providers will shun them and not provide them any services if they think that "cash is king" and that they are masters of the universe.
"Do you use urohydropropulsion by syringing saline to flush back the stones to the bladder and then remove them from the bladder?" I asked him, just in case I can get some tips from his long hours spent in veterinary medicine and surgery. He is likely the most experienced vet in Singapore as he puts in the long hours over 40 years of practice when many vets would have been burnt out or work short hours.
Obviously the most efficient and simple way is to cut a hole into the urethra behind the penile bone and take the stones out. Then stitch up the urethra. Where the complications come in is that the urethra does not close properly and the male Chihuahua will leak urine through this hole, soiling the apartment floor. If the healing is good, the male dog pees normally.
"No point opening up the bladder as there are not stones seen inside," he said. "The bladder is full and any stones inside may not be visible but are likely to be small."
On another matter, I was surprised when he asked me whether the presence of 50 veterinary practices nowadays can be supported by the number of dogs and cats.
He said: "30 years ago, there were only 5 practices - myself, Deveraj, Cho Chak Nam, Animal Clinic and The Veterinary Surgery. I estimated that the number of dogs have increased twice but the number of vet practice has increased 10X. Many dog owners did not license their dogs in the old days. What do you think (of the impact of so many vet practices)?"
"I estimated that the number of dogs would have increased at least 3X based on the number of licences issued and the fact that micro-chipping of dogs is compulsory and enforcement action for unlicensed dogs," I replied. "Some newer vet practices will not be profitable as prices will have to be below costs for such practices in order to attract clientele.
"However, Singaporeans tend to go for proximity and therefore, convenience and affordable costs will bring some business to the new practices and with good personality, some of the newer practices will do very well. Experience and white hairs don't count for most Singaporeans. It is proximity and personality of the younger vets."
I was surprised to see a notice on his reception counter educating members of the public not to be abusive towards his staff. Such notices have been put up by the Singapore General Hospital some 2 years ago but no longer seen and are put up in some government offices or statutory boards like the National Library Board.
Life must be more stressful for some members of the public nowadays such that they become abusive at serving staff. Three Sundays ago, I was on the receiving end of the abusive dog owner who made an appointment to consult Dr Vanessa. He was rude and shouting inside the consultation room where Dr Vanessa and I were present while Dr Vanessa examined his dog's paw. Dr Vanessa kept mum and I left the room, forgetting about the behaviour. At the end of consultation, this man forced his way into the Surgery room where I was consulting with another dog owner and shouted at me to go to the back of the practice and pay him for advice as to what's wrong with my management of Toa Payoh Vets. He was loud and his adult son pulled him away. Such type of clients should be banned and I told Dr Vanessa how to handle such clients in the future. If she keeps silent, she encourages repetition of anger and abuse to me and the staff, except to herself.
Another of Dr Vanessa's client, a young Indian man, punched his fist into the gypsum wall of the consultation room when his family members and him were performing rites on his old dog with oral tumours. The dog had just been put to sleep by Dr Vanessa and the family had prepared some flowers and funeral paraphernalia for the farewell ritual and to wait for the cremation man. Dr Vanessa left the room to attend to another dog at the kennels. I was at the reception area. Suddenly, there was a loud explosive bang on the wall separating the reception from the consultation room. I went inside the consultation room to investigate the bang and since the family was grieving, I did not raise any complaint about the damage.
You can see the dent on the wall when you enter the consultation room of Toa Payoh Vets.
I spoke to Dr Vanessa recently about these two clients of hers. In my 30 years of veterinary practice, I had not encountered such rage. I told her that she had to let such clients know that their behaviour is not acceptable by me, the Principal. If she keeps silent, such behaviour will continue.
"What will you do?" she asked me. "I don't talk to them about their behaviour but focus on consultation."
Well, such anger was not directed at her in the first place. In fact, she was the doctor in charge and consulted. But ignoring such misbehaviour is not good for the team as she obviously cannot work alone. If the vet does not care for the team, the vet should not be accredited to work at Toa Payoh Vets. This is my policy.
This is how she should handle this matter.
I said: "Ask your client courteously - 'Is there some deficiency in my veterinary services to you? How may I help you to improve our veterinary services?"
This is better than keeping silent. I am prepared to ban such abusive clients from Toa Payoh Vets even if they say Dr Vanessa is the best vet in Singapore! Poor anger management is very dangerous to veterinary staff as some angry males do assault and kill. So, it is wise that the Principal or the associate vet know how to handle such clients. Putting up "educational notices" on the walls of Toa Payoh Vets telling clients not to abuse staff is not the answer, in my opinion. This is because the vast majority of Toa Payoh Vets clientele is excellent. The abusive ones make up 1% of the clientele and so I don't permit such "educational notices" to be put up.
The younger generation is into a new golden age of the internet. Those that can manage their anger will prosper. As for those that cannot, the service providers will shun them and not provide them any services if they think that "cash is king" and that they are masters of the universe.
Subscribe to:
Posts (Atom)