"Your dog has at least 4 breast tumours," I said. "How long did the biggest tumour take to grow?"
"Very fast," she said. "In the last month, it just grows so big." The tumour was the size of two golf balls. This was the left MG5 (the left caudal mammary gland, 5th gland)
HOW THIS CASE WAS HANDLED BY ME & DR VANESSA
1. Blood test compulsory.
Total white cell count was over 42 indicating a bacterial infection. I had the dog on IV drip and baytril overnight. Some owners object to blood tests due to financial considerations. X-ray of the chest would be preferred too but this is often not asked of the owner so as to reduce costs.
2. Surgery
Operation to be done the next day due to economic reasons. I prefer wait one week on antibiotics but there are such cases where the owner does not want to wait. Sometimes it may be better to reject such cases but compassion and the interest of the sick dog must be considered by the operating vet.
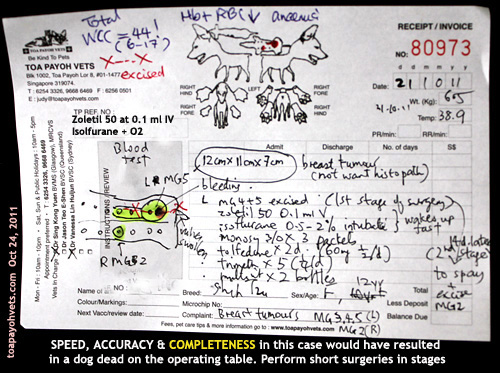
3. Pre-surgery - Zoletil
No sedation preferred. Just use isoflurane gas + oxygen.
Zoletil 0.1 ml IV although Dr Vanessa would have used Domitor. Isoflurane gas + oxygen via mask and then intubation. "Zoletil is safer in old dogs," I said. "Few vets I know use it for small animal sedation."
4. Short surgery
Only the big tumour was excised. This already took around 45 minutes. If the vet attempted to excise all, a dead dog would be the result as old dogs are very high anaesthetic risks.
In a recent on-going court case of a death of a man in his 40s who had liposuction and fat transfer to his chest, the general practitioner (GP) taking 3.5 hours for lipo-suction and transfer of fat to the chest of a man who died, I believe that the whole process of IV anaesthesia (involving topping up) took too long and lead to death. However, there were numerous perforations of the internal organs.
From what I read:
a) The expert witness mentioned about over-sedation as a cause of death as the patient did not respond even though he had numerous internal punctures.
b) The GP doctor doing the liposuction said death was due to fat embolism.
c) The GP doctor doing the IV anaesthesia (Propofol sedation given to effect iv and oxygen, but no general anaesthesia) said that the patient was alive at the end of surgery but died around half an hour later. Therefore anaesthesia was not the cause of death.
d) The autopsy report said death was due to numerous perforations of the intestines and the liver.
e) The judge was exasperated as to why the time and dosages of Propofol had not been made available before the inquest. The info was said to be in the GP's hard disk during the inquest. The case is on-going.
5. Anaesthesia
I was in charge of anaesthesia. The maintenance dose was 0.5 to 1.5% isoflurane. Towards the end of 30 minutes, I showed my assistant Min that the tongue has become white at the edges despite just 1.5%. I reduced to 0.5%. Switched off at the 2nd last stitch. The dog moved a bit. But stitching was done and the dog woke up. This was good anaesthesia. No delay in waking up and no need to use Antisedan as in the case of domitor.
6. Speed of surgery
6.1 Know your anatomy. There is the big blood vessel at around MG3 and MG4. Slow dissection and undermining is OK if you have time but old dog surgery need to be completed in less than 30 minutes for good anaesthetic outcome.
6.2 "No point having a perfect stitching and surgery if the dog dies on the operating table," I said to Dr Vanessa who started stitching up from one end intending to stitch at 0.5 cm intervals as this was her usual method. The wound was around 20 cm long. "Stitch at 1 cm intervals." I also advised stitching at the major points first e.g place 4 stitches and then continue stitching in between.
6.3 "Use walk-in sutures," I explained. But Dr Vanessa was comfortable in using subcuticular sutures to hold the subcutaneous fat together. This took much more time as skin sutures were then sutured with simple interrupted sutures. In "walk-in sutures," I would stitch the skin, then subcutaneous fat and then skin all in one movement using horizontal mattress sutures on the skin.
OUTCOME
The whole process was completed by Dr Vanessa in around 45 minutes. Any longer would have caused death, in my opinion as the tongue was turning pale pinkish cyantotic and white at the edges.
The dog was alive and that was what the owner expected. She had come in the morning of the surgery on Day 2 to ask more questions. I had to be frank as I told her that I needed time to prepare for surgery.
In the evening the happy owner took the dog home. I write this case as a mentoring case done by me.
QUESTIONS ASKED
1. The financial considerations which were addressed yesterday.
2. The chances of survival. Hard to predict as the dog had a bacterial infection and was old at 12 years. Short surgeries make survival likely. So, the other tumours and spaying of the dog had been advised for two weeks later.
3. Whether the breast tumour is cancerous. Most likely as it grows explosively big within a month.
4. Will the tumour come back? Most likely as it is cancerous. However, the owner does not want histopathology by the lab to confirm it.
CONCLUSION
No matter how great the vet surgeon is, anaesthesia is the most important in any surgery as a dog alive is what the owner wants. Beautiful surgery is a bonus.
Toa Payoh Vets webpage is at:
http://www.sinpets.com/F6/20111035old-dog-zoletil-breast-tumours-singapore-toapayohvets.htm
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.