In my review of this recurrent urolithiasis, for the benefit of dog owners, the vet did not perform a stone analysis in the first cystotomy done 12 months ago. This was probably due to the owner's instructions to reduce costs. In the recurrent case, operated by at Toa Payoh Vets by Dr Vanessa, I insisted on a stone analysis. The results were as follows as this ought to be done to know the type of stones present and hence a preventive program using prescription diet or other ways to manage and prevent recurrence.
12.1.12 At Vet 1
after midnight emergency
Shih Tzu, Male, 8 years old
BLOOD TEST
URINE TEST
X-RAY
WBC high 24.48 (5.5 -17)
Neutrophils 82%, L=3.6%, Mono = 12.9%
Absolute High for Neutrophils, Monocytes, Basophils, Platelets, BUN, ALKP.
Dysuria urine pH = 7.2, USG 1.015
3.1.12 at Toa Payoh Vets
SURGERY
URINE TEST
STONE ANALYSIS: Calcium Phosphate.
Urine pH 7.0, USG 1.012
Protein 2+, Blood 4+, WBC 468 RBC 25, Bacteria 3+, Crystals Nil.
Do proper planning before surgery to save on manpower time and resources and to reduce length of anaesthesia, ensuring better survival outcome for old dogs.
No crystals in the urine do not mean no urinary stones inside the bladder or kidneys
Negative for oxalate, urate, magnesium, cystine, ammonia, bicarbonate.
In conclusion, most Singaporean pet owners don't bother with prescription diets, monthly urine tests and 3-monthly X-ray to detect small urinary stones which can be flushed out using urohydropropulsion and thereby saving on surgery and higher costs. However, it is THE DUTY of the veterinary surgeon to record in the case sheet that such advices have had been offered to the owner to prevent misunderstanding when there is a recurrence.
Younger Singaporeans may be much more sophisticated and educated and may understand the need for such preventive tests. But many Singaporeans are time-pressed. Till the dog can't pee or pass blood and then they may consult the vet. I hope this review will provide some information to owners who wants more information on prevention as I do know of some owners who would just euthanase the dog when there is a recurrence.
Website updates and images:
http://www.sinpets.com/dogs/20120219recurrent-urolithiasis-urinary-stones-toa-payoh-vets_Singapore_ToaPayohVets.htm
Wednesday, February 8, 2012
866. Pug needs dry S/D
Today, I phoned owner of a pug to follow up on the pug's fits and why she still needed S/D cans for past few months. The pug has this urinary tract infection if fed home-cooked or other foods.
"SD diet cannot be given for more than 3 months," I advised. "You need to change to CD". I ordered dry CD for her as it is more economical. She had ordered SD diet from a vet in Toa Payoh and when she came, she was told no S/D dry. I made an investigation. S/D dry is not available from the supplier and the vet had not updated her. All vets are to record orders in a book from now.
As the vet in charge, I need to get feedback and this is one such feedback when I followed up with the owner. She had not wanted to "complain" about this lack of service from my associate vet who had promised to order the S/D for her and she came but was told none available.
PUG Male, 3 years
26.1.11 dysuria
23.8.11 Urine test. pH =5 (5-8), SG=1.016 (1.005-1.030.) Nitrite +ve, Bacteria 3+
10.9.11 Urine test pH =8 (5-8), SG=1.029 (1.005-1.030.) Nitrite +ve,
Protein 3+, Ketones trace, Blood 4+, Bacteria 3+. WBC >2250, RBC >2250
Crystals Triple phosphate 2+.
S/D advised.
17.10.11 Urine test. pH =6.5 (5-8), SG=1.006 (1.005-1.030.) Nitrite -ve, Bacteria Nil. Blood trace, WBC 20, RBC 3. Crystals Nil. To acidify urine.
9.9.11 Fits April and Sep 2011. Blood in urine. Follow up today Feb 8, 2012. "One fit episode, no point consulting the vet," she said. I said I was phoning regarding the S/D diet being fed for some time.
10.9.11 Blood test Total WBC high 22 (6-17). N=84% L=7%.
17.10.11 Blood test Total WBC normal but N=10%, L=22%, Monocytes=53%, Basophil =14%. Chronic infection/inflammation likely.
"SD diet cannot be given for more than 3 months," I advised. "You need to change to CD". I ordered dry CD for her as it is more economical. She had ordered SD diet from a vet in Toa Payoh and when she came, she was told no S/D dry. I made an investigation. S/D dry is not available from the supplier and the vet had not updated her. All vets are to record orders in a book from now.
As the vet in charge, I need to get feedback and this is one such feedback when I followed up with the owner. She had not wanted to "complain" about this lack of service from my associate vet who had promised to order the S/D for her and she came but was told none available.
PUG Male, 3 years
26.1.11 dysuria
23.8.11 Urine test. pH =5 (5-8), SG=1.016 (1.005-1.030.) Nitrite +ve, Bacteria 3+
10.9.11 Urine test pH =8 (5-8), SG=1.029 (1.005-1.030.) Nitrite +ve,
Protein 3+, Ketones trace, Blood 4+, Bacteria 3+. WBC >2250, RBC >2250
Crystals Triple phosphate 2+.
S/D advised.
17.10.11 Urine test. pH =6.5 (5-8), SG=1.006 (1.005-1.030.) Nitrite -ve, Bacteria Nil. Blood trace, WBC 20, RBC 3. Crystals Nil. To acidify urine.
9.9.11 Fits April and Sep 2011. Blood in urine. Follow up today Feb 8, 2012. "One fit episode, no point consulting the vet," she said. I said I was phoning regarding the S/D diet being fed for some time.
10.9.11 Blood test Total WBC high 22 (6-17). N=84% L=7%.
17.10.11 Blood test Total WBC normal but N=10%, L=22%, Monocytes=53%, Basophil =14%. Chronic infection/inflammation likely.
Tuesday, February 7, 2012
865. Calcium phosphate urinary stones - Xhih Tzu
Review of one case
Shih Tzu, Male, 8 years old
12.12.10 Dysuria urine pH = 7.2, USG 1.015
12.1.12 At Vet 1 emergency
WBC high 24.48 (5.5 -17)
Neutrophils 82%, L=3.6%, Mono = 12.9%
Absolute High for Neu, Mono, Baso, Plt, BUN, ALKP.
13.1.12
Urine pH 7.0, USG 1.012
Protein 2+, Blood 4+, WBC 468 RBC 25, Bacteria 3+, Crystals Nil
STONE ANALYSIS: Calcium Phosphate.
Negative for oxalate, urate, magnesiu, cystine, ammonia, bicarbonate
Shih Tzu, Male, 8 years old
12.12.10 Dysuria urine pH = 7.2, USG 1.015
12.1.12 At Vet 1 emergency
WBC high 24.48 (5.5 -17)
Neutrophils 82%, L=3.6%, Mono = 12.9%
Absolute High for Neu, Mono, Baso, Plt, BUN, ALKP.
13.1.12
Urine pH 7.0, USG 1.012
Protein 2+, Blood 4+, WBC 468 RBC 25, Bacteria 3+, Crystals Nil
STONE ANALYSIS: Calcium Phosphate.
Negative for oxalate, urate, magnesiu, cystine, ammonia, bicarbonate
864. Performance counts - no repeat consultations
Sheltie, F, 8 years. Copious purulent nasal discharge on left nostril. There might be slight discharge from right nostril.
Feb 7, 2012 visit today. Case handled by Dr Daniel Sing with me. I did mentoring as I have to ensure that service is done efficiently and up to my standard."
It is Feb 7, 2012 now. The 2nd visit was on Jan 7, 2012. Vet 1 had extracted 9 teeth again. But bad breath still remained as I checked the mouth and noted that the gum of M2 on right upper jaw was inflamed. The tooth appeared shaky but I could not confirm it.
What to do with this case? I took over as the man wanted results.
1. Nasal swab for bacteria and fungus. culture and antibiotic sensistivity test.
2. X-ray of nasal area and lung to check for tumours, abscess or infections.
3. Extraction of the loose teeth as bad breath still persisted.
"This is my 3rd visit for the same problem," the owner said. "I want the vet to be pro-active.
The 3-rooted molar on the right upper jaw was shaky and I extracted it within a few seconds. There could be bacteria entering the nasal passages on the right side causing daily mucus production and pus and right nostril discharge. Altogether I extracted 7 teeth.
Will have to wait and see as persistent nasal discharge is hard to treat if it is caused by fungus and/or infected tumours.
Feb 7, 2012 visit today. Case handled by Dr Daniel Sing with me. I did mentoring as I have to ensure that service is done efficiently and up to my standard."
It is Feb 7, 2012 now. The 2nd visit was on Jan 7, 2012. Vet 1 had extracted 9 teeth again. But bad breath still remained as I checked the mouth and noted that the gum of M2 on right upper jaw was inflamed. The tooth appeared shaky but I could not confirm it.
What to do with this case? I took over as the man wanted results.
1. Nasal swab for bacteria and fungus. culture and antibiotic sensistivity test.
2. X-ray of nasal area and lung to check for tumours, abscess or infections.
3. Extraction of the loose teeth as bad breath still persisted.
"This is my 3rd visit for the same problem," the owner said. "I want the vet to be pro-active.
The 3-rooted molar on the right upper jaw was shaky and I extracted it within a few seconds. There could be bacteria entering the nasal passages on the right side causing daily mucus production and pus and right nostril discharge. Altogether I extracted 7 teeth.
Will have to wait and see as persistent nasal discharge is hard to treat if it is caused by fungus and/or infected tumours.
An unusual case: Calcium oxalate stones, then struvite stones 4 months later
This case illustrates the importance of doing urine analysis for urinary stone cases. Sometimes, some vets may not do it to reduce veterinary costs for the owner. This is not good practice unless the owner rejected this test.
FIRST REPORT - SEP 2011 - Calcium oxalate urinary stones
http://www.sinpets.com/F6/20110920retrograde-hydrouropropulsion-singapore_ToaPayohVets.htm. The owner decided to feed just home-cooked food after the surgery.
SECOND REPORT - FEB 2012 - Struvite urinary stones despite giving "home-cooked food".
http://www.sinpets.com/dogs/20120218recurrent-urolithiasis-urinary-stones-calcium-oxalate-struvites-toa-payoh-vets_Singapore_ToaPayohVets.htm

FIRST REPORT - SEP 2011 - Calcium oxalate urinary stones
http://www.sinpets.com/F6/20110920retrograde-hydrouropropulsion-singapore_ToaPayohVets.htm. The owner decided to feed just home-cooked food after the surgery.
SECOND REPORT - FEB 2012 - Struvite urinary stones despite giving "home-cooked food".
http://www.sinpets.com/dogs/20120218recurrent-urolithiasis-urinary-stones-calcium-oxalate-struvites-toa-payoh-vets_Singapore_ToaPayohVets.htm
862. Sunday's interesting case - rabbit eye tearing
Sunday Feb 5, 2012
Bright sunshine. Dr Daniel Sing started his first Sunday of working life after graduation. As a mentor of my associate vets, I was present in this case as in other cases of associate vets. Trust and audit are my management style to ensure a high standard of veterinary care at Toa Payoh Vets and that is why I do intrude into the consultation of my associate vets now and then and review their case sheets. There is no short cuts to be successful in work and life. "Associate vets in Toa Payoh Vets must adopt a consistency in the treatment of similar processes and system to ensure good clinical outcomes," I said to Dr Daniel Sing and Dr Vanessa Lin.
Without a system or standard operating procedure, each vet does his own treatment and may miss out on certain steps. For example, in urolithiasis, a failure to send urine for analysis or stone for analysis unless the client objects to this steps due to economic reasons. So, this is why I am around in some consultations of associate vets.
On this fine Sunday, Dr Daniel had a rabbit which had tearing eyes. A large bald area below the weepy eye. He touched the lower part of this hairless area. I did so too. The rabbit reacted by moving away its face. Abscess or tooth pain?
I got a fluorescein strip from the box and Dr Daniel stained the cornea. Show, not tell is the best in veterinary practice. The rabbit had an eye corneal ulcer as evident by the green 11 o'clock to 2 o'clock stain. So there is an ulcer? What next? New vets tend to relate a list of differential diagnosis to the client, as this is what the vet professors teach them.

5008 - 5009. Corneal ulceration in a rabbit. What is the cure? This is more important than why? The primary cause was two ingrowing cheek teeth on the right side. Isoflurane anaesthesia was necessary to open the mouth as the rabbit was very nervous when the vet tried to open its mouth.
To me, this is OK but some clients just have little time and just want to know what's wrong and the solution. Since this rabbit had an "on-off" eye tearing in the past few weeks and felt pain at the lower maxillary cheek area, Dr Daniel diagnosed teeth problem.
I advised warding the rabbit for one or two days. On the next day, to get the rabbit anaesthesized to check the mouth.
Monday, Jan 6, 2012
Dr Daniel used isoflurane gas mask to anaesthesize the rabbit. Min helped. I was around to pull out the tongue. Inside the left cheek, food and two long curved teeth of around 1.5 cm long were stuck and causing pain. Dr Daniel used the forceps to pull out the two teeth and two broken fragments. I took some images. I quickly irrigate below the 3rd eyelid with 5 ml of clean water as Dr Daniel everted the 3rd eyelid, just in case debris had gone inside it.
The rabbit should feel better now. Will observe on Tuesday and update. Rabbit should be able to go home. "This rabbit eats only pellets", said the gentleman owner. "No hay." He had gone home to bring the rabbit pellets.
Show not tell is the best advice for a vet in private practice. In this case, it was not possible to show the anaesthesia but there were two bone fragments and images to show the owner to give him evidence of what happened and what was done to ensure a good clinical outcome. I don't expect any tearing. On the surface, this appears to be a case of eye corneal injury as there is green fluorescein staining. Veterinary medicine can be challenging. Rabbits can't talk and owners can't tell what's wrong. Therefore, it is up to the vet to palpate (pain in the teeth area) thoroughly and in this case, the primary diagnosis would be ingrowing cheek teeth causing facial pain and irritation and eye rubbing to relieve the pain. A hypothesis. If the rabbit has recovered within 2 weeks, then my hypothesis is correct.
No need to spend money X-raying as visual inspection under anaesthesia using gas mask and isoflurane and oxygen is the method of choice and cheaper. "SC anaesthetic drug injection can be used but not necessary as the gas method is safer and the rabbit wakes up fast," I said.
The cause of tearing of the eye would be due to the rabbit rubbing its facial area to relieve tooth pain of the right teeth cutting into its right cheek, not corneal injury. "This rabbit has to be separated from the other rabbit for some time," I advised the owner. "This is to prevent the other rabbit from grooming or licking its eye." The owner said: "It is difficult to do so." Well, vets should advise but it is up to the owner to accept it.
Updates and more images at:
http://www.sinpets.com/F6/20120217cheek-teeth-ingrown-rabbit-eye-tearing-toa-payoh-vets_Singapore_ToaPayohVets.htm
Bright sunshine. Dr Daniel Sing started his first Sunday of working life after graduation. As a mentor of my associate vets, I was present in this case as in other cases of associate vets. Trust and audit are my management style to ensure a high standard of veterinary care at Toa Payoh Vets and that is why I do intrude into the consultation of my associate vets now and then and review their case sheets. There is no short cuts to be successful in work and life. "Associate vets in Toa Payoh Vets must adopt a consistency in the treatment of similar processes and system to ensure good clinical outcomes," I said to Dr Daniel Sing and Dr Vanessa Lin.
Without a system or standard operating procedure, each vet does his own treatment and may miss out on certain steps. For example, in urolithiasis, a failure to send urine for analysis or stone for analysis unless the client objects to this steps due to economic reasons. So, this is why I am around in some consultations of associate vets.
On this fine Sunday, Dr Daniel had a rabbit which had tearing eyes. A large bald area below the weepy eye. He touched the lower part of this hairless area. I did so too. The rabbit reacted by moving away its face. Abscess or tooth pain?
I got a fluorescein strip from the box and Dr Daniel stained the cornea. Show, not tell is the best in veterinary practice. The rabbit had an eye corneal ulcer as evident by the green 11 o'clock to 2 o'clock stain. So there is an ulcer? What next? New vets tend to relate a list of differential diagnosis to the client, as this is what the vet professors teach them.

5008 - 5009. Corneal ulceration in a rabbit. What is the cure? This is more important than why? The primary cause was two ingrowing cheek teeth on the right side. Isoflurane anaesthesia was necessary to open the mouth as the rabbit was very nervous when the vet tried to open its mouth.
To me, this is OK but some clients just have little time and just want to know what's wrong and the solution. Since this rabbit had an "on-off" eye tearing in the past few weeks and felt pain at the lower maxillary cheek area, Dr Daniel diagnosed teeth problem.
I advised warding the rabbit for one or two days. On the next day, to get the rabbit anaesthesized to check the mouth.
Monday, Jan 6, 2012
Dr Daniel used isoflurane gas mask to anaesthesize the rabbit. Min helped. I was around to pull out the tongue. Inside the left cheek, food and two long curved teeth of around 1.5 cm long were stuck and causing pain. Dr Daniel used the forceps to pull out the two teeth and two broken fragments. I took some images. I quickly irrigate below the 3rd eyelid with 5 ml of clean water as Dr Daniel everted the 3rd eyelid, just in case debris had gone inside it.
The rabbit should feel better now. Will observe on Tuesday and update. Rabbit should be able to go home. "This rabbit eats only pellets", said the gentleman owner. "No hay." He had gone home to bring the rabbit pellets.
Show not tell is the best advice for a vet in private practice. In this case, it was not possible to show the anaesthesia but there were two bone fragments and images to show the owner to give him evidence of what happened and what was done to ensure a good clinical outcome. I don't expect any tearing. On the surface, this appears to be a case of eye corneal injury as there is green fluorescein staining. Veterinary medicine can be challenging. Rabbits can't talk and owners can't tell what's wrong. Therefore, it is up to the vet to palpate (pain in the teeth area) thoroughly and in this case, the primary diagnosis would be ingrowing cheek teeth causing facial pain and irritation and eye rubbing to relieve the pain. A hypothesis. If the rabbit has recovered within 2 weeks, then my hypothesis is correct.
No need to spend money X-raying as visual inspection under anaesthesia using gas mask and isoflurane and oxygen is the method of choice and cheaper. "SC anaesthetic drug injection can be used but not necessary as the gas method is safer and the rabbit wakes up fast," I said.
The cause of tearing of the eye would be due to the rabbit rubbing its facial area to relieve tooth pain of the right teeth cutting into its right cheek, not corneal injury. "This rabbit has to be separated from the other rabbit for some time," I advised the owner. "This is to prevent the other rabbit from grooming or licking its eye." The owner said: "It is difficult to do so." Well, vets should advise but it is up to the owner to accept it.
Updates and more images at:
http://www.sinpets.com/F6/20120217cheek-teeth-ingrown-rabbit-eye-tearing-toa-payoh-vets_Singapore_ToaPayohVets.htm
Monday, February 6, 2012
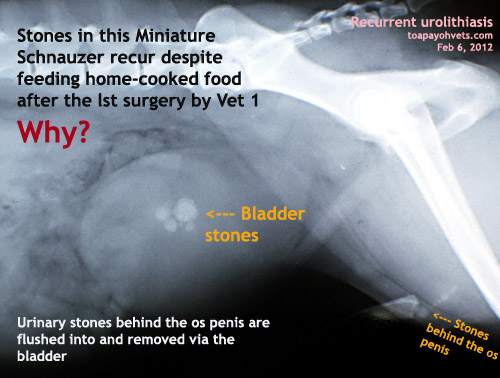
861. Review of recurrent urolithiasis in an 8-year-old lMini Schnauzer
History
Miniature Schnauzer, Male, 8 years
9.3 kg 39.3C
15.9.12 Dysuria >7 days. Eats dry food.
Urethral obstruction. Catheter relieved obstruction.
15.9.12 URINE ANALYSIS
pH=7 (5-8), SG 1.030 (1.005 - 1.030)
Protein +, Blood 4+, WBC 504, RBC 1440, Bacteria +, Crystals Nil
X-ray
BLOOD TEST
Urea = 7 (4.2 - 6.3)
Creatinine = 61 (89-177)
WBC = 13.6 (6-17) with neutrophils 93% absolute 12.6, lymphocytes 6.5%, absolute 0.88
No hypercalcaemia
STONE ANALYSIS - multiple fragmented uroliths. CANINE CALCIUM OXLATE
Calcium oxalaate monohydrate 100% stone 5% shell
Calcium oxalate dihydrate 95% shell
16.9.12 Cystotomy. Urinary stones removed by Vet 1
RECURRENT UROLITHIASIS
3.2.12
8.2 KG 38.4c
Dysuria. Fed home-cooked food.
3.2.12 URINE ANALYSIS
pH=9 (5-8), SG 1.025 (1.005 - 1.030)
Protein 2+, Blood 4+, WBC 0, RBC >2250, Bacteria +, Crystals Triple phosphate +, Amorphous phosphate 3+
STONE ANALYSIS - Sent stones to the lab
Owner did not want blood test
X-rays - 15 stones seen. bladder and behind os penis. see image.
CONCLUSION
This is not a recurrent case of calcium oxalate urinary stones as the 2nd episode showed struvite stone formation.
MANAGING Calcium Oxalate Urolith prevention - do urinalysis and X-rays.
If urine SG >1.020 give canned food or add water to food
If urine pH <6.5, consider diets that produce less acidic urine eg. u/d or use urinary alkalinizers eg. K citrate If urine pH>6.5, USG <1.020, no crystals, repeat urinalysis monthly, then every 3-6 montyhs.
Repeat X-ray every 6-12 months to detect urolith recurrence early.
Repeat urine test and X-rays if signs - haematuria, pollakiuria, dysuria recur.
STRUVITE stones are clinically insignificantg if no urinary tract infection as bacteria forming urease are rquired for struvite urolith formation in dogs.
UROLITHS
1. Voiding urohydropropulsio9n if small uroliths
2. No clinical signs of blood in urine etc, leave stones alone.
3. With persistent signs, remove uroliths
4. Send for stone analysis.
For calcium oxalate prevention,
1. Diets promoting urine pH <6.59 were at highest risk
2. Avoid risk factors like hypercalciuria due to hypercalcemia, metabolic acidosis, high sodium consumption and Vit D excess.
3. Feed canned foods and/or add more water to food so that urine pH is consistently <6.5
4. Consider hydrocholorothiazide (2mg/kg q 12 hr) with highly recurrent urolithaisais in dogs without hypercalcemia.
5. Consider potassium citrate (75mg/kg q 12-24 hr) if urine pH is consistently <6.5
Miniature Schnauzer, Male, 8 years
9.3 kg 39.3C
15.9.12 Dysuria >7 days. Eats dry food.
Urethral obstruction. Catheter relieved obstruction.
15.9.12 URINE ANALYSIS
pH=7 (5-8), SG 1.030 (1.005 - 1.030)
Protein +, Blood 4+, WBC 504, RBC 1440, Bacteria +, Crystals Nil
X-ray
BLOOD TEST
Urea = 7 (4.2 - 6.3)
Creatinine = 61 (89-177)
WBC = 13.6 (6-17) with neutrophils 93% absolute 12.6, lymphocytes 6.5%, absolute 0.88
No hypercalcaemia
STONE ANALYSIS - multiple fragmented uroliths. CANINE CALCIUM OXLATE
Calcium oxalaate monohydrate 100% stone 5% shell
Calcium oxalate dihydrate 95% shell
16.9.12 Cystotomy. Urinary stones removed by Vet 1
RECURRENT UROLITHIASIS
3.2.12
8.2 KG 38.4c
Dysuria. Fed home-cooked food.
3.2.12 URINE ANALYSIS
pH=9 (5-8), SG 1.025 (1.005 - 1.030)
Protein 2+, Blood 4+, WBC 0, RBC >2250, Bacteria +, Crystals Triple phosphate +, Amorphous phosphate 3+
STONE ANALYSIS - Sent stones to the lab
Owner did not want blood test
X-rays - 15 stones seen. bladder and behind os penis. see image.
CONCLUSION
This is not a recurrent case of calcium oxalate urinary stones as the 2nd episode showed struvite stone formation.
MANAGING Calcium Oxalate Urolith prevention - do urinalysis and X-rays.
If urine SG >1.020 give canned food or add water to food
If urine pH <6.5, consider diets that produce less acidic urine eg. u/d or use urinary alkalinizers eg. K citrate If urine pH>6.5, USG <1.020, no crystals, repeat urinalysis monthly, then every 3-6 montyhs.
Repeat X-ray every 6-12 months to detect urolith recurrence early.
Repeat urine test and X-rays if signs - haematuria, pollakiuria, dysuria recur.
STRUVITE stones are clinically insignificantg if no urinary tract infection as bacteria forming urease are rquired for struvite urolith formation in dogs.
UROLITHS
1. Voiding urohydropropulsio9n if small uroliths
2. No clinical signs of blood in urine etc, leave stones alone.
3. With persistent signs, remove uroliths
4. Send for stone analysis.
For calcium oxalate prevention,
1. Diets promoting urine pH <6.59 were at highest risk
2. Avoid risk factors like hypercalciuria due to hypercalcemia, metabolic acidosis, high sodium consumption and Vit D excess.
3. Feed canned foods and/or add more water to food so that urine pH is consistently <6.5
4. Consider hydrocholorothiazide (2mg/kg q 12 hr) with highly recurrent urolithaisais in dogs without hypercalcemia.
5. Consider potassium citrate (75mg/kg q 12-24 hr) if urine pH is consistently <6.5
Subscribe to:
Posts (Atom)