A dermoid is an overgrowth of normal, non-cancerous tissue in an abnormal location. Dermoids occur all over the body. The ones in and around the eye are usually comprised of skin, hair, and/or fat.
WHERE ARE DERMOIDS FOUND AROUND THE EYES?
There are two main dermoid types that occur on or around the eyes.
First, an orbital dermoid is typically found in association with the bones of the eye socket.
Second, an epibulbar dermoid is found on the surface of the eye. There are two typical locations for an epibulbar dermoid. One of the locations is at the junction of the cornea, the clear part at the front of the eye, and the sclera, the white part of the eye. This is a limbal dermoid. The second location of an epibulbar dermoid is on the surface of the eye where the lids meet in the temporal corner (towards the ear) which is often called a dermolipoma or lipodermoid.

The lesion invaded the stromal layer of the cornea, and extended to limbus and conjunctiva. It was surgically resected.
*A pedicle conjunctival flap was placed to support the reepithelization and aid vascularization of the defect.
*After excision, the site where the dermoid lay can be covered by a piece of transplanted cornea.
A third-eyelid flap is also performed to facilitate healing.
After surgery,
An Elizabeth collar to be worn for 2 week.
Eye drops with antibiotics and systemic antibiotics are prescribed for 2 weeks.
*needs operating microscope
Ocular dermoid in a cat.
Treatment: Surgical excision using Surgical Blade No. 11.
The lesion invaded the stromal
layer of the cornea and the sclera at the limbus. The cat was not operated as the owner did not give consent since this was a "stray" cat.
----------------------------------------------------------------------------------
2. A Shih Tzu has a corneal dermoid.
No need to edit. Include the whole footage.
A shih tzu has dermoid in the left eye
----------------------------------------------
3. A labrador retriever has a limbal dermoid.
Give the video link and show some footages of the surgical procedures.
---------------------------------------------------------------------------------------------
Case study of a corneal dermoid in a Shih Tzu
Removal of dermoid by superficial keratectomy is
essential to relieve the related clinical signs (chronic keratitis and epiphora, eye irritation). If the dermoid
has not been totally removed, some degree of recurrence can
be expected [1]. Thus, the dermoid have to excise
completely, if possible, without scarring of the cornea. Once
corneal epithelization is complete, as evidenced by the lack
of fluorescein retention, topical antibiotic-corticosteroid
preparations can be administered to reduce postoperative
corneal scarring and improve the eventual transparency of
the cornea.
After fixation of the globe, abnormal tissue at the conjunctiva
and cornea was removed using the blade (No. 11) and
microsurgical instruments. The lesion invaded by stromal
layer of the cornea, and extended to limbus and conjunctiva
was surgically resected. And then, a pedicle conjunctival
flap was placed to support the reepithelization and aid
vascularization of the defect. Additionally, third-eyelid flap
was also performed to facilitate healing.
-------------------------------------------------------------------------------------------------------
RESEARCH NOTES
VETERINARY DERMOID
Surgical correction of corneal dermoid in a dog
Jae-il Lee1
, Myung-jin Kim1
, Il-hwan Kim2
, Yeoung-bum Kim3
, Myung-cheol Kim1,*
1
Laboratory of Veterinary Surgery, College of Veterinary Medicine, Chungnam National University, Daejeon 305-764, Korea
2
R&D Center of Pharmaceuticals, CJ Corporation, Icheon 467-812, Korea
3
Korea Institute of Toxicology, KRICT, Daejeon 305-343, Korea
A five-month-old female Shih-tzu puppy was presented
for repair of congenital choristoma in left eye. The patient
was suffered from chronic epiphora and ocular discharge
during 3 months. On ophthalmic examination, left eye
revealed hyperemia in conjunctiva of the temporal canthus
due to choristoma with hair. At surgery, the choristoma
invaded by stromal layer of the cornea, and extended to
limbus and conjunctiva. Based on the anatomical location
and histopathological features of the removed tissue, the
choristoma was diagnosed as corneal dermoid.
Key words: choristoma, corneal dermoid, epiphora, hyperemia
Corneal dermoid is a congenital choristoma characterized
by the presence of heterotopic cutaneous tissue in an
inappropriate place [8,4]. They may affect the eyelids,
conjunctiva (palpebral and bulbar), nictitating membrane,
and cornea [3]. This condition is known to occur in large
breed dogs such as St. Bernards [1-3, 7], German Shepherds
[1], short-legged dogs [7] such as Basset Hounds, Dachshunds
and Welsh Corgis and cats [5].
Dermoids contain many of
the elements of normal skin such as epidermis, dermis, fat,
sebaceous glands, hair follicles, and frequently there is hair.
The tissues are usually irritating the eye and associated
structures [3]. Thus, the patients have been suffered from
chronic epiphora and keratitis.
Dermoid may be surgically
excised with complete remission of signs and minimal
scarring of the cornea. This paper describes the incidence of
corneal dermoid and detailed histopathological findings in
shih-tzu dogs.
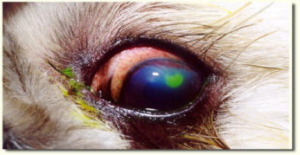
A 5-month-old female Shih-tzu puppy with a weight of
4.4 kg was referred to the Veterinary Medical Teaching
Hospital of Chungnam National University for repair of
congenital choristoma in left eye. The patient had suffered
from chronic epiphora and some ocular discharge during 3
months. On ophthalmic examination, left eye revealed mild hyperemia in conjunctiva at the temporal canthus.
Vital
signs and results of blood examination were within normal
ranges. A light peach color lesion measuring 3-5 mm in
diameter was noted grossly at the limbus in the direction of
5 o’clock, and there was hair growing from the surface (Fig.
1).
The surface of lesion was rough and slightly protruded
compared with the surrounding normal cornea.
The patient was premedicated with atropine sulfate (0.04
mg/kg, SC). Anesthesia was induced with thiopental sodium
(12.5 mg/kg, IV) and maintained with isoflurane. The
patient was administered a balanced electrolyte solution (10
ml/kg/hr, IV), and cefazolin sodium (20 mg/kg, IV) as
prophylactic treatment was administered before surgery.
After fixation of the globe, abnormal tissue at the conjunctiva
and cornea was removed using the sugical blade (No. 11) and
microsurgical instruments.
The lesion invaded the stromal
layer of the cornea, and extended to limbus and conjunctiva
was surgically resected. And then, a pedicle conjunctival
flap was placed to support the reepithelization and aid
vascularization of the defect. Additionally, third-eyelid flap
was also performed to facilitate healing. After surgery, eye
drops as atropine sulfate, gentamicin sulfate, diclofenac
sodium and systemic antibiotics were prescribed for 2
weeks.
For histopathological evaluations, the tissue sample was collected to 10% neutral phosphate-buffed formalin,
processed routinely, and stained with hematoxylin and
eosin.
After 2 weeks, the third-eyelid flap was removed, and the
region of conjunctival flap was epithelized and remained the
scar (Fig. 2). The dermoid hasn’t recurred for 11 months
since the surgical correction, and hyperemia of conjunctiva
and epiphora was disappeared.
Corneal dermoids are ectopic eyelid tissues. They are
nearly always covered with hair. Although, hair may be
removed by manual epilation or electroepilation, it may
regrow. Corneal dermoid has been reported in various
species of animals and in humans, and it is commonly
believed that this disease is generally congenital, although
not hereditary [4]. However, some report in humans, the
appearance of corneal dermoid across three generations of a
single family has been reported by Mattos and his colleagues
[6]. In this case, hereditary pattern was not revealed because
parents were normal ocular structure.
Removal of dermoid by superficial keratectomy is
essential to relieve the related clinical signs. If the dermoid
has not been totally removed, some degree of recurrence can
be expected [1]. Thus, the dermoid have to excise
completely, if possible, without scarring of the cornea.
Once
corneal epithelization is complete, as evidenced by the lack
of fluorescein retention, topical antibiotic-corticosteroid
preparations can be administered to reduce postoperative
corneal scarring and improve the eventual transparency of
the cornea.
Microscopically, it was presented the corneal
dermoid invasive normal corneal epithelium, and the
dermoid contain normal skin such as hair follicles, cornium
and blood vessel (Fig. 3).
The operation of dermoid was delayed in this case due to
owner’s circumstances. Consequently, the lesion was increased
in size and extended more invasively. Fortunately, dermoid
was removed successfully and recurrence did not appear up
to now.
References
1. Gelatt KN. Bilateral corneal dermoids and distichiasis in a
dog. Vet Med Small Anim Clin 1971, 66, 658-659.
2. Gelatt KN. Corneo-conjunctival dermoid cyst in a calf. Vet
Med Small Anim Clin 1972, 67, 1217.
3. Gelatt KN. Pediatric ophthalmology in small animal
practice. Vet Clin North Am Small Anim 1973, 3, 321-333.
4. Horikiri K, Ozaki K, Maeba H, Narama I. Corneal
dermoid in two laboratory Beagle dogs. Exp Anim 1994, 43,
417-420.
5. Lettow E, Teichert G, Pantke G, Leinen U. Eye diseases in
dog and cat 5. A pictorial sequence. Tierarztl Prax. 1974, 2,
299-306.
6. Mattos J, Contreras F, O'Donnell FE Jr. Ring dermoid
syndrome. A new syndrome of autosomal dominantly
inherited, bilateral, annular limbal dermoids with corneal and
conjunctival extension. Arch Ophthalmol 1980, 98, 1059-
1061.
7. Priester WA. Congenital ocular defects in cattle, horse, cats,
and dogs. J Am Vet Med Assoc 1972, 160, 1504-1511.
8. Slatter D. Fundamentals of Veterinary Ophthalmology. 3rd
ed. pp. 208, Saunders, Philadelphia, 2001.
OCULAR DERMOID IN PEOPLE.
The most common location for epibulbar dermoids is the temporal inferior quadrant of the limbus. Though being a benign tumor, the removal of a limbal dermoid is not only performed to improve the cosmetic appearance of the eye but more importantly to prevent loss of visual acuity.
WHAT IS A DERMOID?
A dermoid is an overgrowth of normal, non-cancerous tissue in an abnormal location. Dermoids occur all over the body. The ones in and around the eye are usually comprised of skin, hair, and/or fat.
WHERE ARE DERMOIDS FOUND AROUND THE EYES?
There are two main dermoid types that occur on or around the eyes. First, an orbital dermoid is typically found in association with the bones of the eye socket. Second, an epibulbar dermoid is found on the surface of the eye. There are two typical locations for an epibulbar dermoid. One of the locations is at the junction of the cornea, the clear part at the front of the eye, and the sclera, the white part of the eye. This is a limbal dermoid. The second location of an epibulbar dermoid is on the surface of the eye where the lids meet in the temporal corner (towards the ear) which is often called a dermolipoma or lipodermoid.
WHAT DOES A POSTERIOR EPIBULBAR DERMOID OR DERMOLIPOMA LOOK LIKE?
A posterior epibulbar dermoid is typically yellow in color and soft in consistency, molding to the curve of the eye. The conjunctiva overlying it may be thickened. Occasionally there is one or more hairs sticking out from the mass.
WHERE ARE POSTERIOR EPIBULBAR DERMOIDS (DERMOLIPOMAS) USUALLY FOUND?
Posterior epibulbar dermoids are usually found under the outer upper eyelid in the recess where the eyeball meets the eyelid. Depending on their size, they may be visible only when the upper lid is lifted or if larger they may be seen with the eyelids in the usual position.
DO POSTERIOR EPIBULBAR DERMOIDS NEED TO BE REMOVED?
They rarely require excision. If they are small and not bothersome to the patient or patient’s family, posterior epibulbar dermoids can be left alone.
HOW ARE EPIBULBAR DERMOIDS REMOVED?
Posterior epibulbar dermoids are usually not attached to the eyeball itself. They are attached to the conjunctiva that covers the eye. They often extend posteriorly into the eye socket and usually cannot be entirely removed. Excision involves stripping the dermoid free of the overlying conjuctiva, clamping the mass at the most posterior extent of the dissection and removing the anterior part of the mass. The excised mass is typically sent to a pathologist who can confirm the identity of the tissue.
----------------------------------------------------
WHERE ARE LIMBAL DERMOIDS USUALLY FOUND?
They are found on the surface of the eye either on the cornea or at the junction of the cornea and sclera [See figure 2].
DO LIMBAL DERMOIDS NEED TO BE REMOVED?
Limbal dermoids may be removed to improve the abnormal appearance of the eye and to decrease possible eye irritation.
HOW ARE LIMBAL EPIBULBAR DERMOIDS REMOVED?
The dermoids are removed in a surgical procedure in which the surgeon excises the dermoid from the surface of the cornea and sclera. Sometimes the dermoid extends into the sclera and/or the cornea and care must be taken to avoid entering the eye when excising them. After excision, the site where the dermoid lay can be covered by a piece of transplanted cornea.
DO LIMBAL DERMOIDS CAUSE VISION LOSS?
Occasionally the dermoid is so large that it blocks visual input from entering the eye. More often, vision loss can occur because the presence of the dermoid causes the cornea of the affected eye to have an irregular shape. This warping of the cornea can cause a large amount of astigmatism and a blurred image. The blurred image encourages the developing brain to ignore the input from the affected eye, thus causing vision loss through amblyopia. Fortunately, if amblyopia is detected early during childhood, it can often be successfully treated.
DOES THE RISK OF VISION LOSS GO AWAY AFTER THE DERMOID IS REMOVED?
Not typically. Even though the dermoid is gone, it has often permanently changed the shape of the cornea and the risk of developing amblyopia remains.
ARE LIMBAL DERMOIDS ASSOCIATED WITH OTHER DISEASES?
Yes, sometimes. They can be found in persons with Goldenhar syndrome, linear nevus sebaceous syndrome, and encephalocraniocutaneous lipomatosis, oculoectodermal syndrome, and Townes-Brocks Syndrome.
----------------------------------------------






















No comments:
Post a Comment
Note: Only a member of this blog may post a comment.