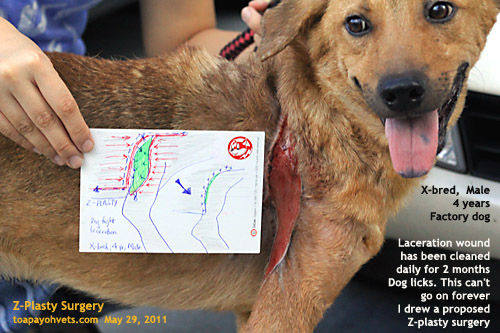
This dog was not under my case and so I did not interfere with the management. Sometimes, the owner has given specific instructions or wishes to impose his or her own instructions on how to manage the dog bite wounds owing to economic considerations. This was not my case as I would have done a Z-plasty if the owner could permit it, at the start of the laceration injury.
Still, I am very concerned about this dog's welfare since his wound is in a high tension area and has not granulated after two months. As each vet treats a case differently according to his or her judgment and the owner's financial consideration, it is hard for the vet sometimes to derive an excellent outcome.
Two months have passed, yet the dog bite laceration wound has not closed. A Z-plasty performed at the beginning may or may not be effective and would be more costly. Still, I would strongly advise the Z-plasty at the start. Due to the high tension and mobile area of the front leg, some thoughts on how to execute the "Z" mark needs to be done.
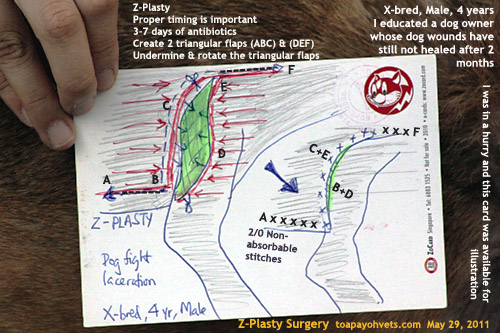
SURGICAL APPROACH 1.
The image above shows one approach to get the "Z" suture pattern.
SURGICAL APPROACH 2.
Another approach is briefly as follows. Consider the wound as a vertical line. Midpoint between the vertical line as a reference guide, use the marker pen to put a "cross (X)" e.g. 5 inches horizontally to the right edge of X. Repeat the procedure horizontally to the left side of the left edge of X.
Make a skin incision from X downwards, to the bottom of the vertical line for the right side, creating a triangular flap. For the left side, make a skin incision from X upwards, creating a triangular flap. When viewed from the front, the cuts look like an "N" unlike the first approach.
Then rotate the two flaps. The final suture pattern will be a horizontal line. In theory, it is easy. In practice, it is difficult and so, daily nursing and cleaning could be the option.
Chemical cauterisation using KMnO4 now may be the most cost-effective solution. The dog can't be kept in the factory for a few months till the granulation tissue takes effect and the dog does not lick the wound.
ECONOMICS
2 months had passed. I advise that the wound by cauterised chemically as it would be relatively costly to do the Z-plasty without a guarantee that the wound will heal normally. This is because the location of the wound is in a high tension mobile skin area.
At the end of the day, much depends on the economics and the recommendation of the vet. Many older owners in the heartland practices, in my opinion, are not too keen on surgery and anaesthesia, due to the higher costs involved and a no-guarantee of successful outcome as in this case. But sometimes, it is penny wise, pound foolish. A younger sophisticated generation may have a different mindset. Still owner education as the illustration in my images will be useful. So far, no practising vet has produced veterinary medical illustrations of common surgeries or that I cannot find a handy book. The medical doctors do have some books on specific parts of the anatomy e.g. piles surgery. I guess there is no income incentive to produce such a book which could also be expensive to buy. However, the internet does help a lot to produce surgery educational videos and illustrations.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.