385. Post-neuter complication - dog traumatises scrotal area
Feedback from a client improves the standard of care
E-MAIL FROM DR SING DATED APRIL 5, 2011 4,52 am
I am Dr Sing from Toa Payoh Vets. We spoke by phone yesterday afternoon. Give the 3 tolfedine tablets before midnight and observe. It is easier to communicate by phone than by texting a reply to your iphone.
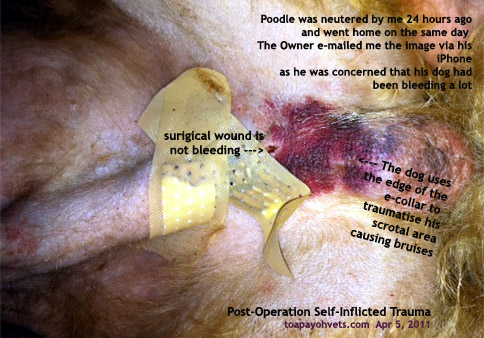
I saw your picture of the dog's scrotal bruising in my phone but since we had just spoken by phone, I did not text a reply back. The dog has been traumatising its scrotal area using the e-collar.
This self-inflicted bruising is one of the post-operation complications seen in a one or two male dogs out of 100. In your dog, the traumatised scrotal skin is not serious presently as it is just 24 hours post-neuter.
Your dog had been given tolfedine pain-killer injection after surgery yesterday morning (Apr 3, 2011). You gave the tolfedine tablets at 4.30 pm on Apr 4, 2011 and noted the redness in the scrotal area. It is good that you e-mail the picture of the site as I thought it was the operation area (which is covered by the plaster) that was bleeding.
As advised, please give 3 tolfedine tablets orally 8 hours after 4.30 pm (your first dose).
Normally, the pain killer should be sufficient but your dog needs twice a day instead of once. Please let me know if your dog needs more pain-killers as normally, I prescribe for around 3 days including the injection post-surgery. Your dog may need an injection if he further traumatise his scrotal area. If not, the redness will fade over 2 weeks. Pl phone me when you have queries as it is much easier to talk than to thumb.
Best wishes.
REVIEW
A small number of male dogs of around 1 in a hundred traumatise their scrotal area after neuter despite being given pain-killer injection post-neuter and oral tablets at home.
In this case, the owner gave the tablets at 4.30 pm, around 24 hours post-surgery. In future, all pets should be given the pain-killers in the morning, ie. 12 hours post-surgery twice a day. Tolfedine is recommended by the manufacturer to be given once a day for a maximum of 4 days. 4 days on, 3 days off schedule. Some vets prefer other brands of pain-killers.
E-MAIL TO DR SING DATED APRIL 6, 2011
Dear Dr Sing
Thank you for your note. We'll continue to observe XXX's conditions over the next few days and contact you again when necessary.
I would also like to highlight that we're very disappointed and frustrated over all the unclear and confusing verbal communications.
When we first pick up XXX post his op, I asked your clinic assistant specifically "when should we feed the medication - morning, afternoon or night? before or after meal?" He said "doesn't matter, just feed once a day."
When we spoke with you last evening, you said specifically "2 tablets 10pm+ or before midnight and 2 tablets again next day morning." which I did feed him 2 tablets at 10pm last night and 2 tablets again this morning. I've 2 tablets left which I'll feed him again tonight.
I believe if XXX is traumatising its scrotal area, its due to itch from the stitches or plasters (which was already loosely attached when we pick up XXX post op). Again, I asked your clinic assistant "when should we remove the plasters or do we need to change to a new one and do we need to bring XXX back to remove stitches or is it the dissolve-able type?" He said "leave the plasters on for next 1-2 days before removing it and don't really need to remove stitches but should bring XXX back to see you in 2 weeks time." which you advised last evening when we spoke "to change a new plaster and leave it on."
Hence, I've a few questions to re-clarify:
1. are the stitches dissolve-able type? if so, is there still a need to see you in 2 weeks time?
2. or if its not, is there any additional charges to remove the stitches on top of the premium price that we've already paid?
3. do we continue to change the plasters when it come loose and leave it on till we see you in 2 weeks time?
4. or can we remove it totally in the next few days?
5. the collar can be removed in 2 weeks time right?
6. both the yellow and pink medication bottles must be fed completely right?
When we first called to inquire about the price, we're advised its $150+ which the final bill came up to a shocking $350+ before you kindly removed the blood test charge of $100 (originally $150 before discount as advised by your clinic assistant) as we did not ask to conduct a blood test. We also found out the general clinics' market rate is $80-$100 for blood test and $5 for the collar which we've been charged $20. I can only hope that the premium price we've paid for is for return of high quality products and professional services to make this whole process most comfortable for XXX's well being.
Appreciate if you can revert on our queries above.
Regards
E-MAIL REPLY FROM DR SING DATED APRIL 6, 2011
It is best to talk directly if you need clarification, whether over the phone or in person. However, I will try and reply to your email queries as detailed as possible below in CAPITAL LETTERS.
On Tue, Apr 5, 2011 at 3:13 PM, ...gmail.com> wrote:
Dear Dr Sing
Thank you for your note. We'll continue to observe XXX's conditions over the next few days and contact you again when necessary.
I would also like to highlight that we're very disappointed and frustrated over all the unclear and confusing verbal communications.
I HAVE SPOKEN TO MY STAFF MR SAW.
When we first pick up XXX post his op, I asked your clinic assistant specifically "when should we feed the medication - morning, afternoon or night? before or after meal?" He said "doesn't matter, just feed once a day."
IN MOST CASES, ONCE A DAY IS THE CORRECT ANSWER AS I HAVE HAD GIVEN THE ANTIBIOTICS AND PAINKILLERS THE AFTERNOON BEFORE. THE NEXT TIMING SHOULD BE 24 HOURS LATER.
I HAVE TOLD MY STAFF TO BE MORE SPECIFIC AND SAY IN THE MORNING.
When we spoke with you last evening, you said specifically "2 tablets 10pm+ or before midnight and 2 tablets again next day morning." which I did feed him 2 tablets at 10pm last night and 2 tablets again this morning. I've 2 tablets left which I'll feed him again tonight.
I believe if XXX is traumatising its scrotal area, its due to itch from the stitches or plasters (which was already loosely attached when we pick up XXX post op). Again, I asked your clinic assistant "when should we remove the plasters or do we need to change to a new one and do we need to bring XXX back to remove stitches or is it the dissolve-able type?" He said "leave the plasters on for next 1-2 days before removing it and don't really need to remove stitches but should bring XXX back to see you in 2 weeks time." which you advised last evening when we spoke "to change a new plaster and leave it on."
IF PLASTER IS LOOSE, IT NEEDS TO BE CHANGED. THE PLASTER IS TO FURTHER PREVENT THE DOG FROM LICKING THE WOUND AND STITCHES
Hence, I've a few questions to re-clarify:
1. are the stitches dissolve-able type? if so, is there still a need to see you in 2 weeks time?
NO NEED TO SEE ME TO REMOVE THE STITCHES AS THEY ARE ABSORBABLE. STITCHES WILL DISSOLVE IN 14-28 DAYS TIME. BUT IN SOME CASES, THE STITCHES DO NOT DISSOLVE IN 14 DAYS' TIME AND THE DOG IS IRRITATED BY ITS PRESENCE, I ASK THE OWNER TO COME AND GET THEM REMOVED FREE OF CHARGE.
2. or if its not, is there any additional charges to remove the stitches on top of the premium price that we've already paid?
NO ADDITIONAL CHARGES
3. do we continue to change the plasters when it come loose and leave it on till we see you in 2 weeks time?
CHANGE THE PLASTER WHEN IT IS LOOSE OR DIRTIED
4. or can we remove it totally in the next few days?
IN SOME CASES, YES. MUCH DEPENDS ON THE DOG'S SENSITIVITY TO HAVING A PLASTER ON. I CANNOT BE SPECIFIC AS EACH DOG BEHAVES DIFFERENTLY AFTER SURGERY, TOWARDS THE PAIN AND IRRITATION OF WOUND HEALING
5. the collar can be removed in 2 weeks time right?
PREFERRED BUT IN SOME CASES, 1 WEEK WILL DO. MUCH DEPENDS ON THE DOG'S BEHAVIOUR TOWARDS WOUND HEALING. SOME DOGS ARE VERY SENSITIVE AS WOUND HEALING AREA IS IRRITATING BUT SOME DON'T BOTHER.
6. both the yellow and pink medication bottles must be fed completely right?
YES
When we first called to inquire about the price, we're advised its $150+ which the final bill came up to a shocking $350+ before you kindly removed the blood test charge of $100 (originally $150 before discount as advised by your clinic assistant) as we did not ask to conduct a blood test.
AS YOU DID NOT WANT THE BLOOD TEST TO BE DONE, MY ASSISTANT SHOULD DEDUCT $150. IF NOT, I WILL REFUND YOU BACK BY CHEQUE $50. I WILL ASK HIM TODAY.
We also found out the general clinics' market rate is $80-$100 for blood test and $5 for the collar which we've been charged $20. I can only hope that the premium price we've paid for is for return of high quality products and professional services to make this whole process most comfortable for XXX's well being.
MARKET RATE FOR BLOOD TEST VARIES. YOUR BLOOD TEST IS A COMPLETE BLOOD TEST WHICH INCLUDES HAEMATOLOGY AND TESTS INCLUDING THE FUNCTIONS OF LIVER, KIDNEY, BONES AND JOINTS, GLUCOSE LEVEL. IT IS NOT POSSIBLE TO COMMENT FURTHER BASED ON PRICES OF COMPETITORS. AS FOR THE E-COLLAR, PRICES VARY AND IT IS BEST YOU PHONE ME IF YOU WISH TO DISCUSS FURTHER THE PRICING.
YOUR DOG'S REACTION TO NEUTER IS NOT COMMON BUT DOES HAPPEN IN 1 OUT OF 100 CASES. IT IS NOT SERIOUS AS HE HAS THE PAIN-KILLER TOLFEDINE. TOLFEDINE IS RECOMMENDED TO BE GIVEN ONCE A DAY FOR 4 DAYS ON, 3 DAYS OFF. SINCE YOUR DOG HAS SENSISTIVITY TO PAIN, I ADVISED TWICE A DAY ON THE DAY YOU PHONED.
I HOPE ALL ARE WELL WITH HIM NOW. PL PHONE RATHER THAN TEXT AS IT IS MUCH CLEARER TO TALK THAN TO WRITE AS MISUNDERSTANDINGS ARE LIKELY TO OCCUR DURING WRITING.
E-MAIL TO DR SING DATED APRIL 7, 2011
Thanks for your notes. It's very helpful info and clarifies. There's no need for refund of blood test as all blood test charges has been taken out at point of payment.
E-MAIL FROM DR SING DATED APR 6, 2011
I spoke to my assistant whose last day is today. He said that it was $100 which was charged in the bill but had been taken out.
I appreciate your feedback as that is the most important way to improve my standard of management and service. There is no other way as the practice learns from experience and mistakes made. The best feedback are those that I have made mistakes. Will update instructions post-surgery to all my vets with a standard form now. Pl accept my thanks.
E-MAIL TO DR SING DATED APR 6, 2011
I hope my feedback didn't cause Mr Saw his job, that will be too harsh.
Good thinking, I'm sure your clients will appreciate a standard FAQ surgery fact sheet for their reference. This should save you answering repetitive queries and able you to focus on other matters.
Regards
We will continue to observe XXX's recovery from here.
E-MAIL FROM DR SING DATED APRIL 7, 2011
Thanks for your feedback. Mr Saw completed his 3-year contract. He has better prospects of starting his own practice in Yangon. He has had done an excellent job during his employment and left on very good terms with his employer. I will be doing the surgery fact sheet with my two other associate vets as all 3 of us have different post-operation nursing care and advices. For example, I use plaster to cover the surgical wound to prevent it from being contaminated by the environment and licking by the dog or cat. My associate vets do not but use the e-collar.
I hope your dog is OK now. Thank you.
CONCLUSION
The vet usually explains the risks and post-operation complications. The owner is also asked to sign the Toa Payoh Vets' Informed Consent Form to confirm he or she has been informed of the risks and complications.
Risks refer to the anaesthetic risks. Therefore a blood test is advised to confirm that the dog is healthy. Post-operation complications are pain, bleeding and infection and are listed in the Informed Consent Form.
In 99% of the neuter and spay cases in my 30 years of small animal practice in Toa Payoh Vets, there have rarely been complaints of post-op complications at Toa Payoh Vets as I prescribe antibiotics and pain killers post-surgery. I do have a post-surgical information fact sheet but it has not been given as a routine.
A very small number of dogs have low tolerance to pain after neuter or spay. Some vets even give pain-killer injections before surgery as well as after. A post-surgical advice sheet will be best.
I will get this post-operation complication advices information incorporated in the spay or neuter certificate to be printed officially and signed by the owner so that the information has been read and is always available for family members.
Phoning the vet at Toa Payoh Vets is still the best way to get answers to queries of post-op complications although text messages and e-mails to me are very common with the younger generation.
THE WEBPAGE IS ALSO AT:
http://www.kongyuensing.com/folder5/20110325Trauma_self-inflicted-scrotal-post-neuter-dogs-surgery-toapayohvets.htm